

Publication
Research Article
International Journal of MS Care
Environmental Factors Affecting the Daily Functioning of Jordanian Individuals with Multiple Sclerosis
Occupational therapists must consider the hindering and facilitating effects of the environment on patients' functional performance when planning therapeutic interventions. The purpose of this study was to explore environmental factors that hinder, and available services that facilitate, the daily functioning of Jordanian individuals with multiple sclerosis (MS) as perceived by the patients themselves. A sample of 103 Jordanian individuals with MS completed a questionnaire on hindering environmental factors and facilitative services. Factors and services were identified according to their description in the World Health Organization's International Classification of Functioning, Disability and Health. Environmental factors that were reported by the participants to be most hindering to their daily functioning were stores and malls (74.2%), noise (87.1%), attitudes of immediate family (52.0%), and government policies and regulations (52.2%). Moreover, the participants reported that psychological services were the least available facilitative services in the community (83.8%). Weak-to-moderate but significant correlations were found between a number of demographic variables and perceived hindering factors. The study results indicate that hindering factors, facilitative services, and demographic variables should be given greater attention by rehabilitation practitioners (especially occupational therapists) when planning intervention programs for Jordanian individuals with MS.
Multiple sclerosis (MS) is a devastating chronic neurologic disorder that affects millions of people worldwide.1 Its chronic and unpredictable trajectory often results in debilitating physical and cognitive impairment affecting daily functioning and may have devastating effects on patients' quality of life and well-being.2 3
Given that MS often strikes individuals at their peak productive age of 20 to 40 years,4 5 multidisciplinary rehabilitation programs (eg, comprising physical, occupational, and speech therapy) to manage the effects of the disease on functioning are essential for these people.6–8 Among these programs, occupational therapy is typically aimed at minimizing disability, maximizing independence in activities and participation, and preventing future disability.9 10 This usually requires a systematic functional assessment that addresses all areas of one's life. The World Health Organization's International Classification of Functioning, Disability and Health (ICF) best describes this systematic assessment,11 depicting human health and functioning as the result of a dynamic interaction among several health-related domains.12 Each domain is an integral part of the interaction and thus should be considered when assessing functional performance.
According to the terminology used by the ICF, assessment conducted for patients with MS traditionally includes detecting impairment in body functions and structures, either physical (eg, fatigue, weakness, poor balance, pain) or cognitive (eg, difficulties in memory and executive functions). It also includes assessing limitations in daily activities (eg, functional mobility, self-care, work, leisure), restrictions on participation (eg, involvement in interpersonal relations and social events), and contextual factors (eg, physical and social environment). Thus the ICF systematic representation of human functioning can be a helpful guide for physicians and therapists not only in assessment but also when planning medical and rehabilitative interventions for people with MS. Occupational therapists typically use this systematic approach because holistic treatment is a core concept in both traditional and contemporary occupational therapy theories and practice worldwide.13 Therefore, occupational therapists using the ICF as a model may find it easier to communicate with physicians and other rehabilitation therapists when planning interventions for people with MS.14
There is a growing body of research on the relationship between the clinical impairment seen in MS and health-related areas of activities and participation.4 15–17 However, there is limited focus on the effect of contextual—namely, environmental—factors on functioning in this population.7 18 The environment surrounding an individual, in its physical or social sense, may contain several factors characterized as enabling (eg, good transportation services or family support), disabling (eg, lack of good transportation services or unsupportive family members), or neutral (eg, availability of transportation services when there is no need for any, or neutral family attitudes) with respect to one's performance of daily activities. Although the relationship between these factors and the individual's performance is complex, the influence of the factors usually depends on the individual's health status. The healthier and more functional the individual is, the less likely he or she is to be affected by the disabling factors in the environment. On the other hand, the more disabled the individual is, the more likely he or she is to be affected by such disabling environmental factors. Therefore, the ICF describes environmental factors as facilitating or hindering to the individual's performance. The factors are defined as the “physical, social and attitudinal environment in which people live and conduct their lives.”12 (p16) Physical environments or societies containing barriers may hinder one's performance, while those without barriers may facilitate one's performance.12 Thus an essential part of assessing one's performance is investigating the effect of environmental factors that may be hindering or facilitating daily functioning, in order to identify areas for intervention.
Given the complexity of “environment” as a construct, the body of research in this area is very limited. Several studies have been conducted to explore ICF environmental factors in different disease populations,19 20 but only one study by Prodinger et al.7 explored the effect of environmental factors as described in the ICF, focusing on Austrian patients with MS. The study used a cross-sectional survey to describe patient-perceived disability in relation to ICF environmental factors in 101 community-dwelling individuals with MS. The results showed that products related to mobility (eg, regular cars), attitudes of immediate and extended family, and limited social and health-care resources were the most hindering environmental factors with regard to functional activities such as mobility, work, household activities, and social life participation.
The ICF includes both aspects of the physical environment and societal attitudes as integral parts of the environment, and it is clear that certain factors such as economy, policies, and social norms will vary tremendously across different countries and cultures. Consequently, environmental factors may differ in their hindering or facilitating impact on patients' daily functioning, especially for those with long-term disabling conditions such as MS. For instance, developing countries such as those in the Middle East tend to have fewer resources in terms of the economy, research, and health-care systems compared with developed countries such as the United States. Moreover, great differences may be found across developed and developing countries in terms of societal beliefs about health and disability, traditions, norms, and religious orientation. Accordingly, the effect of environment in countries with limited resources is especially important for occupational therapists both locally and internationally in their research and clinical practice.
Not only is research on the effect of the environment on daily functioning of individuals with MS scarce worldwide, but no such studies have been reported in developing countries, where medical and health-care resources tend to be less available, especially for those with chronic illnesses such as MS. Thus such a study was conducted in Jordan, a developing Middle Eastern country with a population of 6 million. Jordan has limited health-care resources given that the sector has a budget of only 7.5% of gross domestic product. Also, like other Arabic countries, Jordan features a culture that is family-oriented and conservative in terms of traditions, religion, and social habits. Therefore, a person with MS in Jordan may be greatly affected by a number of environmental factors. The purpose of this study was to explore the effect of environmental factors described in the ICF on the daily functioning of Jordanian individuals with MS as perceived by the patients themselves.
Methods
Participants
A convenience sample of individuals with MS was recruited from the Jordan Society for Multiple Sclerosis to participate in this study. The society is a nonprofit national association that advocates for the rights of MS patients from all regions in Jordan and provides basic services for its members such as medical insurance, medications, and some rehabilitation services (eg, physical therapy sessions). People with MS from all Jordanian regions are represented in the society. Ethical approval for conducting the study was obtained from the Scientific Research Committee of the society. The inclusion criteria for participants were an official diagnosis of MS made at least 6 months previously, and the ability to comprehend and respond to questions in the questionnaire. The exclusion criteria were the presence (or comorbidity) of other chronic physical illness or disability (eg, stroke or spinal cord injury), a diagnosis of mental illness, psychotic symptoms, or severe cognitive impairment.
The Questionnaire
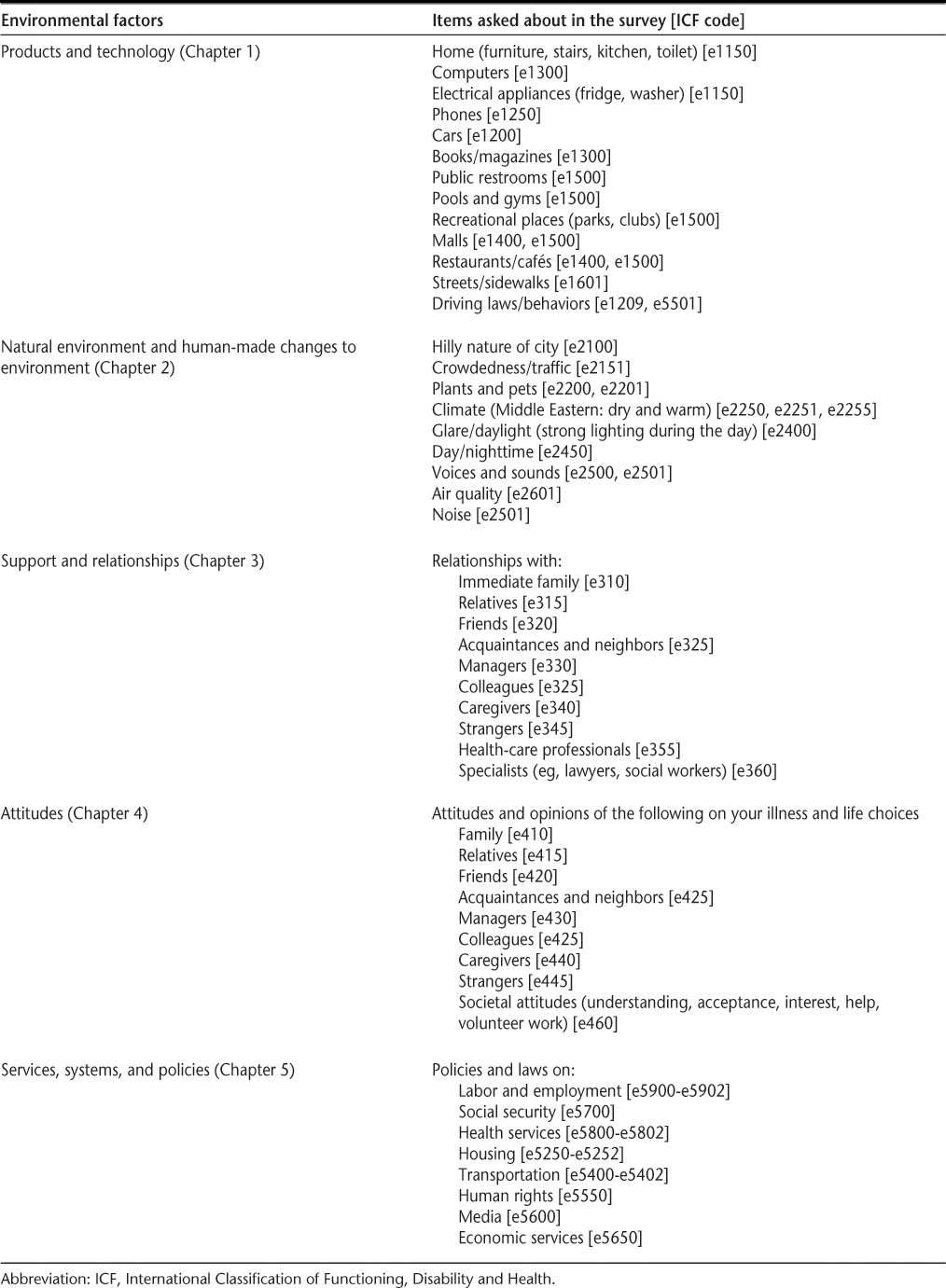
A questionnaire was distributed to the study participants to explore two issues. The first issue was the extent to which individuals perceived certain environmental factors as hindering to their daily functioning. Daily functioning was defined as “performance in important daily activities such as self-care, functional mobility, and household activities” (given that these activities seem to be of the greatest importance to people with MS).21 Environmental factors were considered to be aspects of the Jordanian physical or geographic environment, culture, or society that could affect the individual's daily functioning. Factors were derived from the ICF chapters (in the section “Environment”) on products and technology (Chapter 1), natural environment and human-made changes to environment (Chapter 2), support and relationships (Chapter 3), attitudes (Chapter 4), and services, systems, and policies (Chapter 5). To determine the environmental factors and services to be included in the questionnaire (Table 1), a panel of three occupational therapists (two with doctoral degrees and one with a bachelor's degree) was formed. First, the panel reviewed the content of all five ICF chapters in the section “Environment” and identified specific examples described in each chapter. Then, the panel discussed and agreed on possible relevant factors and services in the Jordanian community that were consistent with the content of each chapter. For each chapter, a number of phrases describing specific examples of environmental factors were listed, and the study participants were asked to evaluate the hindering effect of these factors on daily functioning (eg, mobility, self-care). For example, 18 phrases describing products and technology (eg, furniture, stairs, kitchen, bathroom, appliances) represented Chapter 1; 9 phrases describing components of Jordan's nature, climate, and geography represented Chapter 2 (eg, sunny, hot, and dry weather and hilly nature of the city); 11 phrases describing relationships represented Chapter 3 (eg, immediate family, relatives, friends, colleagues, strangers); 8 phrases describing attitudes and opinions of individuals surrounding the participants (eg, family, friends, government, and community) represented Chapter 4; and finally, 1 phrase describing a number of policies and government regulations represented Chapter 5 (eg, labor legislation and social security services).


Barriers to daily functioning as classified and coded in the ICF
Part 1: Perceived Hindering Environmental Factors
For this part of the questionnaire, the participants were asked to rate the degree to which the listed environmental factors hindered their daily functioning. The specific wording was “determine the level of disability or difficulty imposed by each of the following factors on your daily functioning in important daily activities especially when taking into account the problems and symptoms caused by multiple sclerosis.” Participants had to rate each item on a 5-point scale (1 = not hindering at all; 2 = minimally hinders functioning or 25% of the time; 3 = moderately hinders functioning or 50% of the time; 4 = severely hinders functioning or 75% of the time; 5 = entirely hinders functioning or 100% of the time).
For analysis purposes, the percentages of participants who rated the factors 2 through 5 were combined (ie, the percentages of patients reporting the environmental factors to be hindering 25% to 100% of the time). Moreover, factors were reported here only if they were identified as hindering by at least half of the participants, to reflect the majority's perspective. Descriptive statistics were used for the analysis. The panel considered this 50% cutoff point appropriate given the great subjectivity of participants' perceptions of the “level of hindering or difficulty” and the broad range of MS-related impairment among the participants.
After completion of data analysis for the first part of the questionnaire, further bivariate correlation analyses were conducted to explore the association between demographic variables (eg, age, duration of illness) and the reported hindering factors (if any). Pearson correlation coefficients were used for this purpose.
Part 2: Perceived Availability of Services and Community Support
Part 2 of the questionnaire explored the participants' perceptions of the availability of services and support described in the ICF chapter on services, systems, and policies (Chapter 5) that may facilitate daily functioning. Fourteen questions asked about services, systems, or policies affecting the daily functioning of the participants (eg, legislation, medical insurance, psychological and religious support, community awareness). For this part, participants used a different 4-point scale (1 = unavailable; 2 = available but very limited; 3 = available; 4 = abundantly available) to rate the availability of services or community support that may facilitate their daily functioning. Examples of services included medical services (eg, medical insurance, counseling, social services), transportation (eg, buses and taxis), human rights advocates, media, rehabilitation services (physical and occupational therapy), economic and financial support (eg, social security, recruiting agencies), psychological support (eg, support groups, religious support, spiritual support), and attitudes of community members (eg, understanding, acceptance, support, and volunteer work provided by individuals in the community for the MS population). For this part, the percentages of patients reporting that services were unavailable (score 1) or available but limited (score 2) were combined. Again, only items identified by at least half of the participants as unavailable were reported in this study using descriptive statistics.
The questionnaire also inquired about participants' demographic information such as age, gender, education, marital status, duration of illness, employment, and income. A cover letter was directed to the participants explaining the purpose of the study, encouraging the participants to answer all questions if possible, and emphasizing the confidentiality of identifying data. Completing the questionnaire took 10 to 15 minutes on average. All data collected from the questionnaire were analyzed using SPSS, version 16 (SPSS Inc, Chicago, IL).
Results
Participants
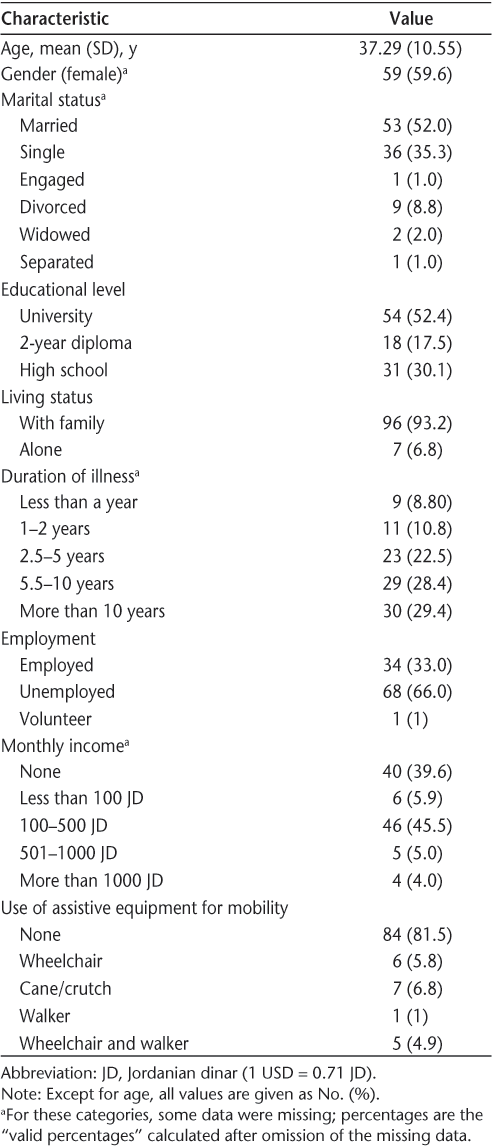
A total of 103 people with MS filled out the questionnaire. Most of the participants were female (59.6%), married (52.0%), and living with family (93.2%). Moreover, most were unemployed (66.0%), had a university-level education (52.4%), and had an illness duration of over 5 years (57.8%). All participants were initially diagnosed with the relapsing-remitting type of MS. While most patients (n = 84) used no assistive equipment for ambulation or functional mobility, 6 used a wheelchair, 7 used a cane or a crutch, 1 used a walker, and 5 used both a wheelchair and a walker. The demographic characteristics of the sample are shown in Table 2.


Demographics of the study participants (N = 103)
Part 1: Perceived Hindering Environmental Factors
Products and Technology (ICF Chapter 1)
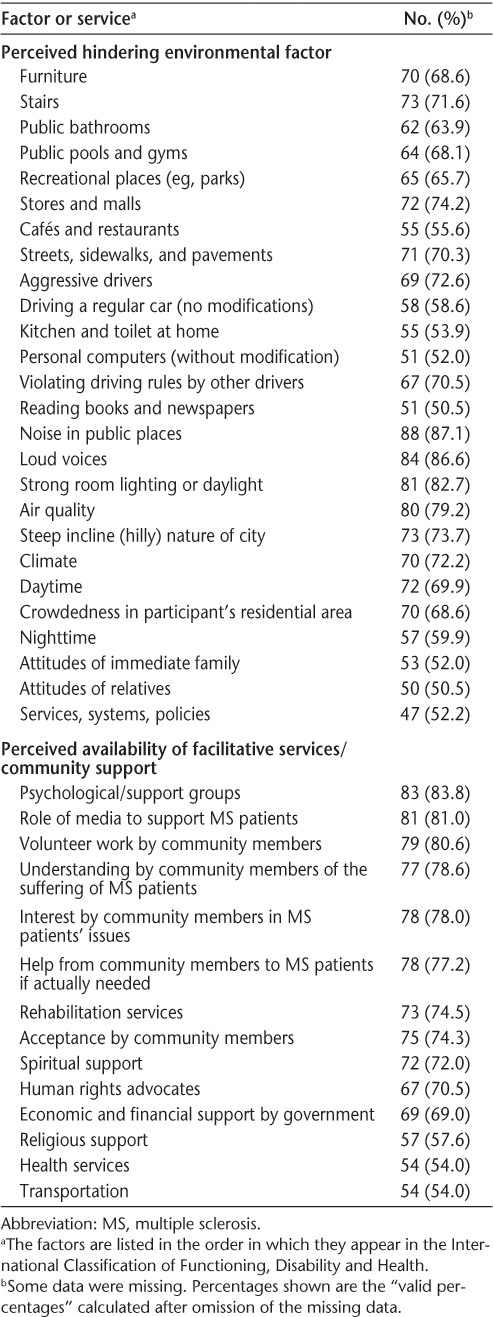
The numbers and percentages of patients reporting that their daily functioning was hindered by factors in the category “products and technology” were as follows: stores and malls, 72 (74.2%); aggressive drivers, 69 (72.6%); stairs, 73 (71.6%); violating driving rules by other drivers (eg, blocking, speeding), 67 (70.5%); streets, sidewalks, and pavements, 71 (70.3%); home furniture, 70 (68.6%); public pools and gymnasiums, 64 (68.1%); recreational places (eg, parks), 65 (65.7%); public bathrooms, 62 (63.9%); driving a regular car (ie, no modifications), 58 (58.6%); cafés and restaurants, 55 (55.6%); kitchen and toilet at home, 55 (53.9%); personal computers without modifications, 51 (52.0%); reading books and newspapers, 51 (50.5%) (Table 3).


Perceived hindering environmental factors and availability of facilitative services in the study sample (N = 103)
Natural Environment and Human-Made Changes to Environment (ICF Chapter 2)
The numbers and percentages of patients reporting that their daily functioning was hindered by factors in the category “natural environment and human-made changes to environment” were as follows: noise in public places (eg, in malls), 88 (87.1%); loud voices, 84 (86.6%); strong room lighting or daylight, 81 (82.7%); air quality, 80 (79.2%); steep incline (hilly) nature of the city, 73 (73.7%); climate, 70 (72.2%); daytime, 72 (69.9%); crowdedness in participant's residential area, 70 (68.6%); nighttime, 57 (59.9%) (Table 3).
Support and Relationships; Attitudes; Services, Systems, and Policies (ICF Chapters 3–5)
No items in the “support and relationships” category were perceived as hindering for the participants. In the category “attitudes,” 53 (52.0%) and 50 (50.5%) participants reported that their daily functioning was hindered by the opinions and perspectives of immediate family members and relatives, respectively. In the category “services, systems, and policies,” 47 (52.2%) reported that their daily functioning was hindered by certain policies and government regulations (Table 3).
Correlations Between Demographic Variables and Hindering Factors
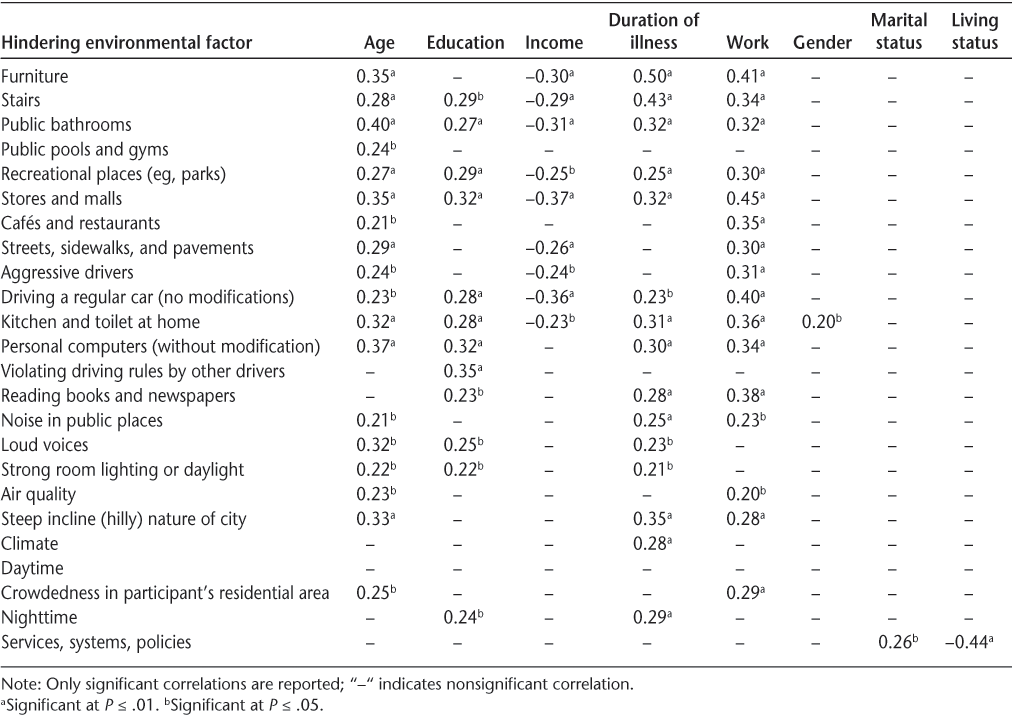
All correlations found between the demographic variables and perceived hindering environmental factors were weak to moderate but significant. The strongest correlations were found between age and public bathrooms (r = 0.40, P ≤ .01); duration of illness and furniture (r = 0.50, P ≤ .01), duration of illness and stairs (r = 0.43, P ≤ .01); work and furniture (r = 0.41, P ≤ .01), work and stores and malls (r = 0.45, P ≤ .01), work and driving a regular car (r = 0.40, P ≤ .01), and finally living status and services, systems, and policies (r = −0.44, P ≤ .01). All significant correlations are shown in Table 4; nonsignificant correlations were not reported in this study.


Significant bivariate Pearson correlations between demographic variables and hindering environmental factors as perceived by the participants
Part 2: Perceived Availability of Services and Community Support (ICF Chapter 5)
The services and support reported most frequently to be unavailable were psychological/support groups (n = 83, 83.8%), followed by the role of media to support MS patients (n = 81, 81.0%), volunteer work by community members to help MS patients (n = 79, 80.6%), understanding by community members of the suffering of MS patients (n = 77, 78.6%), interest by community members in MS patients' issues (n = 78, 78.0%), help by community members to MS patients if actually needed (n = 78, 77.2%), rehabilitation services (n = 73, 74.5%), acceptance by community members (n = 75, 74.3%), spiritual support (n = 72, 72.0%), human rights advocates (n = 67, 70.5%), economic and financial support by government (n = 69, 69.0%), religious support (n = 57, 57.6%), health services (n = 54, 54.0%), and transportation (n = 54, 54.0%) (Table 3).
Discussion
The purpose of this study was to explore hindering environmental factors and determine the availability of services that can facilitate the daily functioning of Jordanian individuals with MS as perceived by the individuals themselves.
The results showed that the factors in the category “products and technology” that were perceived by the participants to be most hindering to daily functioning were public places (eg, stores and malls, public bathrooms, pools, parks, sidewalks, cafés and restaurants) and actions of other people (eg, aggressive drivers, violating driving rules by other drivers). The least hindering factors were items controlled by the individual himself or herself (eg, home furniture, kitchen, computers) and activities conducted by the individual himself or herself (eg, reading books and newspapers). This indicates that the physical environment (largely represented by products and technology), especially the part that is shared with other people, may represent a major barrier for people with MS. The finding that the physical environment is most hindering when it is shared with or controlled by other people is especially noteworthy and should encourage health-care practitioners—especially occupational therapists, who are most involved in environmental modifications—to pay special attention to the people sharing the physical environment with patients. It also highlights the importance of raising the awareness of family and community members about their possible negative effects on the person with MS and encouraging them to examine their behaviors to avoid further burdening the patient. The results for the “products and technology” category are consistent with the findings of Prodinger et al.7 that products intended for public use (eg, stairs and crosswalks) were rated by Austrian patients with MS as moderately to highly important for work and social participation.
Even more interesting are the results for the category “natural environment and human-made changes to environment.” Noise in public places and loud voices topped the list of factors hindering daily functioning of MS patients in this category (over 85% of the sample). Once again, this highlights the hindering effect of the public on the daily functioning of these patients. Although other characteristics such as strong room lighting, air quality, climate, and the hilly nature of the city were also rated high for their hindering effect on daily functioning (consistent with the findings of Prodinger et al.7), factors imposed by people were most disturbing to the participants. This finding is interesting because nature-related factors might be expected to be perceived by patients as most hindering given the neurologic impairment inherent to MS, which results in sensitivity to sunlight and temperature changes.
Interestingly, over half of the participants reported that the attitudes and perspectives of people closest to them (immediate family, 52.0%; relatives, 50%) were among the most hindering factors—similar to the results of Khan and Pallant for Australian patients with MS.2 Moreover, slightly more than half (52.2%) of the participants reported that official policies and governmental regulations hindered their daily functioning. These results are puzzling given that patients usually complain about governmental services (or the lack of them), rather than attitudes of their immediate or extended families. Thus it is noteworthy that a majority of participants reported family as a hindering factor, especially in a family-oriented culture such as Jordan's.
Although most of the reported correlations in this study were weak to moderate, all of them were significant. Thus demographic variables—especially age, education, duration of illness, income, and work—can influence patients' perceptions of the hindering effect of the surrounding environment. For instance, older individuals usually have longer durations of illness and may have more physical and cognitive impairment, which may make them more vulnerable to the actual or perceived hindering effect of the environment (eg, public bathrooms, furniture, and stairs). Other demographic variables may also amplify the actual or perceived hindering effect of the environment. For example, being less educated may result in fewer employment opportunities (especially in a developing country such as Jordan) and consequently in lower income, which limits the ability of the patient to pay for environmental modifications (eg, to a car) or afford certain expenses (eg, shopping at malls). Hence, when treating patients with MS, health-care professionals must consider the contributing effects of demographic variables on the individuals' disability and attempt to distinguish such effects from those of the environment or the illness itself. This delineation will help professionals plan a comprehensive intervention that takes into account all factors in the patient's life that may affect his or her disability. Furthermore, other significant (though statistically weaker) correlations found in this study, such as that between gender and kitchen activities, indicate that health-care professionals must consider the effect of all variables on the performance of daily activities. The results from the correlation analyses are generally consistent with the findings of Gulick22 that personal attributes (eg, age, education, illness duration) and the availability of social support affected the performance of daily activities (eg, personal care) in US patients with MS despite the presence of emotional stress caused by the illness itself.
The results of the second part of the questionnaire showed that at the top of the list of unavailable or available but very limited services was psychological support, followed by the role of the media to support MS patients and then community-related factors (acceptance, understanding, and volunteer work by community members) and rehabilitation services. Again, the role of the community and its members seems to be a key factor affecting the daily functioning of individuals with MS.
The results for the importance of rehabilitation services to Jordanian individuals with MS are similar to those found by Coenen et al.23 in Dutch MS patients and by Prodinger et al.7 in Austrian MS patients; in both of those studies, rehabilitation services were reported as important to patients' daily functioning and quality of life. This is important to consider in terms of the medical services provided for this population. It is noteworthy that although technical services (eg, health, economic and financial, and transportation) were reported to be limited by more than half of the participants, they were not perceived as the most unavailable types of services. Services that target patients' well-being (eg, psychological support, spiritual support, and human rights advocates) and those contributed by the community (eg, role of media; acceptance, understanding, and volunteer work by community members) were perceived to be more important than technical services in facilitating daily functioning.
The clinical implications of the results are that occupational therapists, other health-care practitioners, and decision makers in the health-care sector must pay more attention to the physical aspects of the environment, particularly those affected or shared by other people in the community. Greater efforts to provide services that target the well-being of MS patients and increase the awareness and contributions of community members will eventually facilitate the daily functioning of this population.
Limitations of this study include the small sample size, the inclusion of patients with only one type of MS (the relapsing-remitting type), and the lack of standardized outcome measures to assess the level of functional disability of the participants. Thus future studies should include a wider range of participants with identified levels of disability.
In conclusion, this study showed that environmental factors, especially those involving other people, can be major obstacles to MS patients' daily functioning. Greater attention should be paid to these factors, as well as to basic services provided in the rehabilitation process for people with MS.
PracticePoints
Jordanian individuals with MS perceive public places and activities shared with other people as most hindering to their daily functioning.
Family attitudes are also perceived to negatively affect daily functioning; thus integrating patients' family members into the rehabilitation process is important.
Demographic variables such as age and duration of illness may contribute to the perceived hindering effects of the environment.
Psychological support is perceived to be one of the most important services needed by Jordanians with MS for improved daily functioning.
References
Rosati G. The prevalence of multiple sclerosis in the world: an update. Neurol Sci. 2001; 22: 117–139.
Khan F, Pallant JF. Use of the International Classification of Functioning, Disability and Health (ICF) to identify preliminary comprehensive and brief core sets for multiple sclerosis. Disabil Rehabil. 2007; 29: 205–213.
Wynia K, Middel B, van Dijk JP, De Keyser JHA, Reijneveld SA. The impact of disabilities on quality of life in people with multiple sclerosis. Mult Scler. 2008; 14: 972–980.
Benito-León J, Morales J, Rivera-Navarro J, Mitchell A. A review about the impact of multiple sclerosis on health-related quality of life. Disabil Rehabil. 2003; 25: 1291–1303.
McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the Diagnosis of Multiple Sclerosis. Ann Neurol. 2001; 50: 121–127.
Khan F, Turner-Stokes L, Ng L, Kilpatrick T. Multidisciplinary rehabilitation for adults with multiple sclerosis. Postgrad Med J. 2008; 84:385.
Prodinger B, Weise AP, Shaw L, Stamm TA. A Delphi study on environmental factors that impact work and social life participation of individuals with multiple sclerosis in Austria and Switzerland. Disabil Rehabil. 2010; 32: 183–195.
Stevenson VL, Playford ED. Rehabilitation and MS. Int MS J. 2007; 14: 85–92.
Law M. The environment: a focus for occupational therapy. Can J Occup Ther. 1991; 58: 171–180.
Wade DT, de Jong BA. Recent advances in rehabilitation. BMJ 2000; 320: 1385–1388.
Arthanat S, Nochajski S, Stones J. The International Classification of Functioning, Disability and Health in its application to cognitive disorders. Disabil Rehabil. 2004; 26: 235–245.
World Health Organization. ICF: International Classification of Functioning, Disability and Health. Geneva: World Health Organization; 2001.
Stamm TA, Cieza A, Machold K, Smolen J, Stucki G. Exploration of the link between conceptual occupational therapy models and the International Classification of Functioning, Disability and Health. Aust Occup Ther J. 2006; 53: 9–17.
Stucki G, Ewert T, Cieza A. Value and application of the ICF in rehabilitation medicine. Disabil Rehabil. 2002; 24: 932–938.
Buchanan RJ, Huang C, Kaufman M. Health-related quality of life among young adults with multiple sclerosis. Int J MS Care. 2010; 12: 190–199.
Freeman JA. Improving mobility and functional independence in persons with multiple sclerosis. J Neurol. 2001; 248: 255–259.
Isaksson AK, Ahlström G, Gunnarsson LG. Quality of life and impairment in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry. 2005; 76: 64–69.
Rimmer JH. Use of ICF in identifying factors that impact participation in physical activity/rehabilitation among people with disabilities. Disabil Rehabil. 2006; 28: 1087–1095.
Whiteneck G, Meade M, Dijkers M, Tate D, Bushnik T, Forchheimer M. Environmental factors and their role in participation and life satisfaction after spinal cord injury. Arch Phys Med Rehabil. 2004; 85: 1793–1803.
Threats T. Access for persons with neurogenic communication disorders: influences of personal and environmental factors of the ICF. Aphasiology. 2007; 21: 67–80.
Lexell EM, Iwarsson S, Lexell J. The complexity of daily occupations in multiple sclerosis. Scand J Occup Ther. 2006; 13: 241–248.
Gulick E. Emotional distress and activities of daily living functioning in persons with multiple sclerosis. Nurs Res. 2001; 50: 147–154.
Coenen M, Basedow-Rajwich B, König N, Kesselring J, Cieza A. Functioning and disability in multiple sclerosis from the patient perspective. Chronic Illn. 2011; 7: 291–310.
Financial Disclosures: The author has no conflicts of interest to disclose.








