

Publication
Research Article
International Journal of MS Care
Potential of Timed 25-Foot Walk Values in Predicting Maximum Walking Distance in Persons with Multiple Sclerosis
Abstract
Background:
Expanded Disability Status Scale (EDSS) scores of 4.0 or greater are determined primarily by maximum walking distance (MWD). Estimation of MWD by persons with multiple sclerosis (MS) is often used due to the impracticality of formally walking a person with MS in a clinic setting. Previous studies have demonstrated discrepancies between estimated and actual MWDs. Whether Timed 25-Foot Walk test (T25FW) values can be used to predict MWD is currently unknown. This study aimed to determine whether T25FW time is predictive of MWD in persons with MS.
Methods:
This study is a post hoc analysis of a previously described prospective cohort study. Persons with MS with an EDSS score of 3.5 to 5.5 were included. The participant’s T25FW values and MWD were measured.
Results:
Of the 38 adult participants (mean age, 50.8 years; 27 women [71%]), 24 (63%) had relapsing-remitting MS. The median EDSS score was 4.5 (range, 3.5–5.5). The T25FW times were divided into seven categories (<5.0, 5.0–5.9, 6.0–6.9, 7.0–7.9, 8.0–8.9, 9.0–9.9, and ≥10.0 seconds). The MWDs were divided into corresponding EDSS score categories: ≥500, 300–499, 200–299, 100–199, and ≤99 m. Ordinal logistic regression, when controlled for age, found the T25FW categories to be predictive of EDSS score (χ2 = 17.630, df = 7, P = .014).
Conclusions:
The T25FW value may be used as a surrogate estimate of MWD. Further studies are needed to confirm the reliability of the T25FW in predicting MWD.
Multiple sclerosis (MS) is a chronic debilitating neurologic disease most often diagnosed in young individuals. Several instruments are used to assess disease progression; however, the most widely used instrument in clinical practice and in trials is the Expanded Disability Status Scale (EDSS).1 The EDSS is used to evaluate the functional status of different neurologic domains and is an ordinal scale ranging from 0 (normal neurologic status) to 10 (death due to MS) in 0.5-point increments (after the first step of 1.0 from EDSS score 0 to EDSS score 1.0). The lower EDSS scores measure impairment based on the neurologic examination, and the upper range of the scale (EDSS scores >6.0) is dictated by the use of walking aids or level of dependency. Scores between 4.0 and 6.0 are mostly dictated by walking ability. For example, if a person with MS has a maximum walking distance (MWD), without walking aid or rest, of greater than 500 m but not unlimited, their EDSS score will be 4.0 regardless of the absence of any disability in other functional domains. For EDSS scores of 4.5, 5.0, and 5.5, MWD is 300 m, 200 m, and 100 m, respectively. For an EDSS score of 6.0, the person with MS can walk for 100 m with unilateral aid or assistance.1 , 2 Therefore, accurate estimation of walking ability is essential to calculate the EDSS score correctly. Incorrect scoring of the EDSS can have negative consequences, as coverage for disease-modifying therapies is often dictated by EDSS score. Furthermore, it could lead to unnecessary treatment changes or inaccurate evaluation of disease progression. Previous studies have demonstrated that patients are not always able to accurately report the best walking distance, as shown in orthopedic and vascular studies.3 – 5 We also previously demonstrated that persons with MS do not accurately estimate their maximum walking, and this wrong estimation affects the EDSS score in 44% of cases.2 Measuring MWD in persons with MS at each visit is not always practical because it is time-consuming. Therefore, an alternative way to estimate MWD is needed.
In contrast, the Timed 25-Foot Walk test (T25FW) is a measure of the time in seconds that a person with MS needs to walk 25 feet as fast and as safely as they can.6 The T25FW is a component of the Multiple Sclerosis Functional Composite.7 The T25FW is one of the most commonly used objective measures of walking and can be applied in a wide range of persons with MS with variable walking abilities. The T25FW is much easier to administer in the clinical setting compared with MWD.8 It is unknown whether T25FW values can be used to predict MWD. This study aims to determine whether T25FW values are predictive of MWD, and thus EDSS scores, in persons with MS.
Methods
Study Population
This work is a post hoc analysis of the proportion of persons with MS with EDSS scores of 3.5 to 5.5 from a previously described prospective cohort study.2 Participants were patients with MS who were seen for routine medical care in an academic MS clinic at a tertiary care hospital in London, Ontario, Canada.
The inclusion and exclusion criteria were as previously described.5 Persons with MS were included as follows: 1) any subtype of MS (relapsing-remitting, secondary progressive, or primary progressive) and 2) age 18 to 64 years. In the original study, persons with MS with EDSS scores of 3.5 to 7.0 were included. In the present study, we also excluded individuals with walking aids (EDSS score, 6.0–7.0) to allow for a homogeneous sample when examining T25FW times. The exclusion criteria were as follows: 1) any comorbid conditions affecting walking, such as cardiac disease, respiratory disease, and arthritis; 2) peripheral neuropathy due to any other illness; 3) fampridine therapy start in the past 6 months; and 4) relapse in the past 3 months. Information was collected regarding participants’ type of MS, time since diagnosis, date of the most recent relapse, and full medication history, including use of disease-modifying therapies.
T25FW Measurement and Categorization
For each participant, as previously described, T25FW values were measured, and MWD was then measured along a prespecified walking course. We categorized T25FW values in two ways: Method 1 consisted of seven categories: <5.0, 5.0–5.9, 6.0–6.9, 7.0–7.9, 8.0–8.9, 9.0–9.9, and ≥10.0 seconds), and method 2 consisted of three categories (< 6.0, 6–7.9, and ≥8.0 seconds).
In method 1, T25FW values were categorized based solely on convenience as a change of 1 second intuitively indicates a change. Method 2 was selected based on the study by Goldman et al,9 which provided some evidence of T25FW benchmarks that were clinically meaningful, specifically related to occupational and social changes. Persons with T25FW times of 6.0 to 7.9 seconds are more likely to have occupational disability or to change their job because of walking disabilities.9 A T25FW time of 8.0 seconds or more was associated with being more likely to be dependent in daily living activities and requiring social and governmental health care and support.9
The MWDs were divided into their EDSS score equivalents (MWD-EDSS): ≥500, 300–499, 200–299, 100–199, and ≤99 m.
Statistical Analysis
Ordinal logistic regression was used to determine the predictive value of T25FW categories on MWD-EDSS. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp, Armonk, NY).
The study protocol was approved by the University of Western Ontario (London, ON, Canada) Health Sciences Research Ethics Board; all the participants provided written informed consent before participation.
Results
The 38 participants included in this analysis had a mean age of 50.8 (range, 41–59) years. Most of the participants self-reported as women (27 [71%]) and as White race (33 [87%]). Twenty-five participants (66%) had relapsing-remitting MS, ten (26%) had secondary progressive MS, and three (8%) had PPMS. The mean time since diagnosis was 11.5 (range,1–35) years. The baseline characteristics of the study population are shown in Table 1.


Baseline characteristics of the 38 study participants
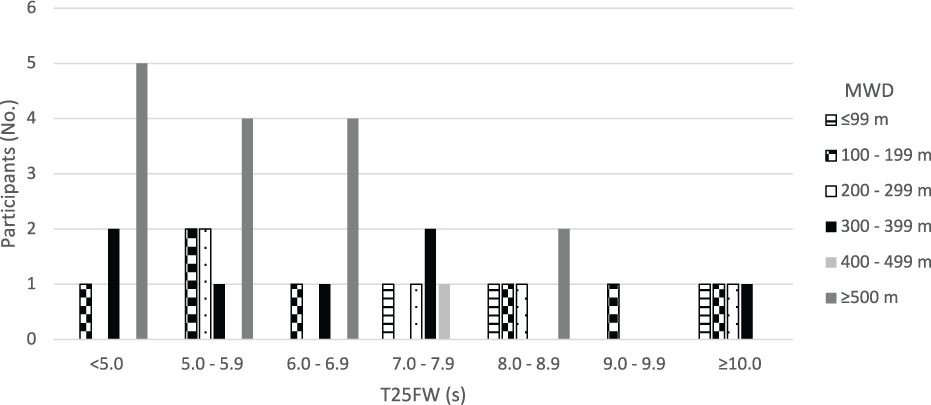
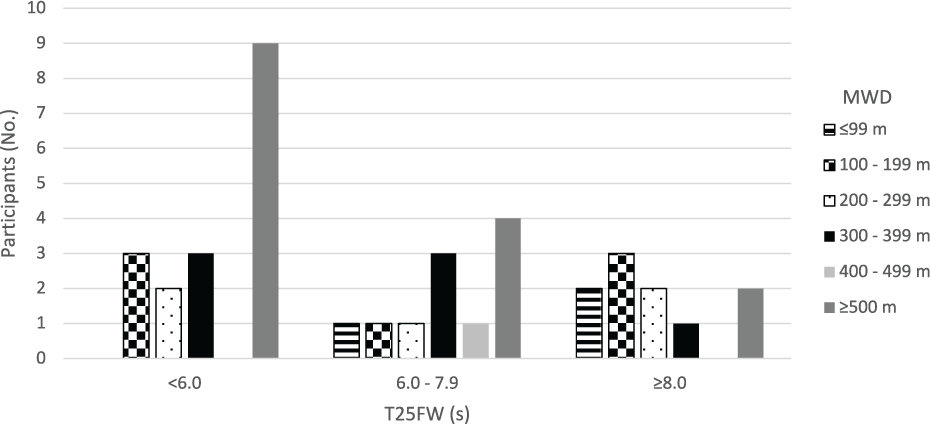
Ordinal logistic regression, when controlled for sex, found the T25FW categories divided as in method 1 to be predictive of MWD-EDSS (χ2 = 17.630, df = 7, P = .014) (Figure 1). For method 2, ordinal logistic regression, when controlled for sex, found that these T25FW categories were also predictive of MWD-EDSS (χ2 = 8.678, df = 3, P = .034) (Figure 2).


Relationship between maximum walking distance (MWD) and Timed 25-Foot Walk test (T25FW) value using method 1


Relationship between maximum walking distance (MWD) and Timed 25-Foot Walk test (T25FW) value using method 2
Discussion
The present study shows that T25FW time could predict MWD in persons with MS. A correct or exact EDSS score estimation is vital because it can affect eligibility for treatment. Most persons with MS have some mobility problems,7 and thus it is essential to determine their best MWD accurately. Accurate serial EDSS score measurement is also crucial in follow-up of individuals with MS because it can lead to changes in pharmacologic management or a diagnosis of progressive MS, which may lead to treatment restriction by the insurance company. Minor changes in EDSS scores could be of high concern, especially in persons with MS with higher EDSS scores, as suggested by the Canadian Multiple Sclerosis Working Group.10 For example, persons with MS and an EDSS score of 5.5 who had an increase of 0.5 in their EDSS score within 6 months require serious consideration for treatment escalation as suggested by the Canadian Multiple Sclerosis Working Group.10
Flawed perception of distances by patients and physicians has also been proved in other fields of medicine; a test to estimate the distance of an object placed at a specified distance results in inaccurate estimation by both patients and vascular surgeons.11 A study by Giantomaso et al4 of patients referred to rehabilitation with some walking disabilities for a variety of medical reasons showed that neither patients nor physicians are accurate in estimating MWD and that patients usually overestimate and physicians underestimate the distances that patients can walk. Our previous study examined the accuracy of estimated MWD in persons with MS. Persons with MS were asked to estimate their MWD, and then MWD was tested actually by asking them to walk their maximum. Only 56% of persons with MS were able to accurately estimate their MWD.2 Another important point is that MWD in persons with MS can vary from day to day, making it more challenging to estimate MWD because it should reflect the best function of the patient.12 Therefore, the T25FW, which is a reliable and valid test8,13 and has been used as the primary end point in clinical trials,14 offers a better alternative to estimate MWD and, subsequently, EDSS score based on the results of the present study.
To our knowledge, this is the first study to suggest that the T25FW can predict MWD in persons with MS and, therefore, predict their EDSS score. Further studies are needed to determine whether T25FW values can be used as surrogate estimates of MWD. Among the limitations to this study are the small sample size and use of a convenience sample from a specialized MS clinic, which could affect generalization of the results. Participants were tested on a single occasion only; fatigue, distress, and time of day might affect ability to walk in persons with MS, and these potential confounders may be challenging to take into account when estimating MWD. Another point is that this discussion mainly applies to use of the EDSS score in clinical practice. Patient estimates of MWD are not allowed in clinical trials. We focused on a specific EDSS score range (3.5–5.5), and, therefore, the present findings cannot be generalized to the full range of EDSS scores.
In conclusion, physicians should be aware that self-reported MWD may be inaccurate when estimating EDSS score. The T25FW could predict the patient’s MWD and provide a reliable objective estimation of walking capacity. However, further studies are needed to confirm the reliability of the T25FW in predicting MWD.
PRACTICE POINTS
Expanded Disability Status Scale (EDSS) score is heavily dependent on correct estimation of maximum walking distance (MWD) in persons with MS.
Some persons with MS do not accurately estimate their MWD, which leads to inaccurate changes in EDSS scores.
The Timed 25-Foot Walk test can be used as a convenient method to predict MWD and can lead to more accurate EDSS scores.
Financial Disclosures
Dr Berger is a consultant for Roche, EMD Serono, Sanofi Genzyme, Biogen, and Novartis and an advisory board member for Roche and Novartis. Dr Morrow has, in the past 3 years, served on advisory boards for Biogen, EMD Serono, Sanofi Genzyme Canada, Novartis, and Roche; has received investigator-initiated grant funds from Biogen, Novartis, and Roche; and has acted as site principal investigator for multicenter trials funded by Novartis, Genzyme, Roche, Adamas, and AbbVie. The other authors declare no conflicts of interest.
References
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an Expanded Disability Status Scale (EDSS). Neurology. 1983; 33: 1444– 1452.
Berger W, Payne MWC, Morrow SA. Self-reported maximum walking distance in persons with MS may affect the EDSS. J Neurol Sci. 2017; 379: 77– 80.
Duprez D, de Backer T, de Buyzere M, Clement DL. Estimation of walking distance in intermittent claudication: need for standardization. Eur Heart J. 1999; 20: 641– 644.
Giantomaso T, Makowsky L, Ashworth NL, Sankaran R. The validity of patient and physician estimates of walking distance. Clin Rehabil. 2003; 17: 394– 401.
Meyer-Moock S, Feng YS, Maeurer M, Dippel FW, Kohlmann T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014; 14: 1– 10.
Rudick RA, Cutter G, Reingold S. The Multiple Sclerosis Functional Composite: a new clinical outcome measure for multiple sclerosis trials. Mult Scler. 2002; 8: 359– 365.
Cutter GR, Baier ML, Rudick RA, . Development of a multiple sclerosis functional composite as a clinical trial outcome measure. Brain. 1999; 122( pt 5): 871– 882.
Bosma L, Kragt JJ, Polman CH, Uitdehaag BMJ. Walking speed, rather than Expanded Disability Status Scale, relates to long-term patient-reported impact in progressive MS. Mult Scler. 2013; 19: 326– 333.
Goldman MD, Motl RW, Scagnelli J, Pula JH, Sosnoff JJ, Cadavid D. Clinically meaningful performance benchmarks in MS. Neurology. 2013; 81: 1856– 1863.
Freedman MS, Selchen D, Arnold DL, . Treatment optimization in MS: Canadian MS Working Group updated recommendations. Can J Neurol Sci. 2013; 40: 307– 323.
Watson CJ, Collin J. Estimates of distance by claudicants and vascular surgeons are inherently unreliable. Eur J Vasc Endovasc Surg. 1998; 16: 429– 430.
Albrecht H, Wotzel C, Erasmus LP, Kleinpeter M, Konig N, Pollmann W. Day-to-day variability of maximum walking distance in MS patients can mislead to relevant changes in the Expanded Disability Status Scale (EDSS): average walking speed is a more constant parameter. Mult Scler. 2001; 7: 105– 109.
Hobart J, Blight AR, Goodman A, Lynn F, Putzki N. Timed 25-Foot Walk: direct evidence that improving 20% or greater is clinically meaningful in MS. Neurology. 2013; 80: 1509– 1517.
Goodman AD, Brown TR, Krupp LB, . Sustained-release oral fampridine in multiple sclerosis: a randomised, double-blind, controlled trial. Lancet. 2009; 373: 732– 738.








