

Publication
Research Article
International Journal of MS Care
Effects of a Single Bout of Aquatic Exercise on Mood in Multiple Sclerosis
Abstract
Background:
Physical activity is known to be an effective way of managing multiple sclerosis (MS)–related symptoms. Furthermore, it has been reported that even a single bout of physical activity can yield improvements in mood in persons with MS. Aquatic exercise can be an effective and enjoyable physical activity in persons with MS. However, there is little research on the immediate effects of aquatic exercise on mood in people with MS. Thus, we assessed the acute effects of a single bout of aquatic exercise on mood.
Methods:
Eight adults with MS participated in a 45-minute aquatic exercise class as well as 45 minutes of a seated rest control condition. The Profile of Mood States questionnaire was given before and after each condition (rest and aquatic exercise). Repeated-measures analysis of variance and paired-samples t tests were used to examine whether aquatic exercise resulted in improvement in mood. Due to the small sample size, effect sizes were considered.
Results:
Moderate-to-large effect sizes indicated a condition × time interaction such that mood increased and fatigue decreased after a single bout of aquatic exercise compared with after rest.
Conclusions:
This proof-of-concept study suggests that mood symptoms are improved immediately after a short bout of aquatic exercise. Future research is needed to explore whether these effects are reliable and whether they can be sustained with more frequent bouts of aquatic exercise.
Most persons with multiple sclerosis (MS) experience mood disturbances,1 which can have a major effect on quality of life (QOL).2 Exercise training (ET) interventions have been highlighted as a promising approach for managing hallmark symptoms in persons with MS, such as mood3 and fatigue,4 as well as for improving QOL.5 However, the mechanism by which ET exerts beneficial effects on mood is not well understood. Most research studies have focused on the effects of long-term ET (weeks to months).6–8 Although research has indicated that ET can improve mood after extended exposure, limited research has examined the effect of ET on acute mood symptoms in persons with MS. For example, it is not known whether mood improvements after ET require multiple repeated sessions or whether they can be experienced immediately after exercise. Only a handful of studies to date have examined the effects of acute bouts of exercise in persons with MS,9–11 and these studies have reported mostly positive outcomes, including improvement of mood and cognition.10 However, no studies, to our knowledge, have expanded this investigation of short-term exercise to aquatic exercise and, thus, the present study examined mood changes after a single bout of aquatic exercise.
Aquatic exercise has been recommended by the American Physical Therapy Association for people with MS to improve disabling symptoms and problems associated with sedentary lifestyles.12 The existing literature is scarce regarding the effects of aquatic exercise in persons with MS, despite the advantages it may provide compared with nonaquatic ET.13 Those advantages are related to three properties of water. First, the buoyancy of water, which results in the reduction of body weight in water, makes it easier and safer for people with disabilities to move without assistance. Second, the viscosity of water increases the amount of resistance, which makes aquatic exercise a form of resistance training. Finally, the conduction of water may reduce body temperature (if the temperature of the water is kept at 80°F–84°F, the recommended temperature for persons with MS), thus enabling persons with MS to prolong training sessions without the fear of overheating.13
To date, studies on aquatic exercise in people with MS have focused mostly on its effects on QOL,14 fatigue,15 balance,16 mobility and strength,16 and pain.17 Only one study, to our knowledge, has examined mood specifically after an aquatic exercise intervention, and it reported substantial benefit.15 Thus, more studies are needed to replicate and confirm this finding. Furthermore, no studies, to our knowledge, have examined mood changes after an isolated bout of aquatic exercise to examine whether the benefit is immediate. Our hypothesis is that similar to what has been found in nonaquatic exercise,10 mood will improve after a single bout of aquatic exercise. To examine the hypothesis, we used the Profile of Mood States (POMS) questionnaire because this was used in the previous study to examine the effects of a single bout of nonaquatic exercise10 to see whether the findings could be replicated using the same measure. Due to a small sample size that limits the ability to reach statistical significance, we considered effect sizes in interpreting the findings.
Methods
Participants
Eight participants with definite MS based on the criteria of Polman et al18 were enrolled. Participants were included if they were aged 18 to 65 years, were inactive in their daily life (ie, completed ≤30 minutes of exercise per week in the past 6 months as reported during the telephone interview), and were fluent English speakers. We screened for inactivity 1) to ensure homogeneity related to baseline activity levels in the sample and 2) because those who are inactive were most likely to experience benefit from a single bout of exercise. Participants were excluded if they had a history of substantial substance abuse and/or neurologic disease other than MS or major significant psychiatric illness. Furthermore, participants were excluded if they had experienced a relapse within 1 month before enrollment or during the study.
Procedure
Recruitment and enrollment were performed between January 1, 2015, and May 31, 2019. The institutional review board at Kessler Foundation (East Hanover, NJ) approved the study. Persons with MS were recruited through a database provided by Kessler Foundation. Potential participants were phoned for an initial screening and were asked to provide basic information related to age and previous neurologic, psychiatric, and substance abuse history. All potential participants completed a written informed consent form before their involvement in the study. Individual numeric identifiers were assigned to each participant at the time of enrollment to ensure confidentiality.
Aquatic Exercise Versus Rest
Mood was assessed before and after two conditions: aquatic exercise and rest. The aquatic exercise condition consisted of 45 minutes of supervised aquatic exercise that incorporated stretching and toning exercises focused on improving flexibility, balance, and strength and mild-moderate aerobic activity. Participants were newly enrolled in an aquatic exercise group class as part of a larger study to examine the effects of aquatic exercise on multiple outcome measures (findings to be published separately). The 45-minute class was led by an instructor certified by the National Multiple Sclerosis Society and the Aquatic Therapy & Rehab Institute (Naples, FL). The outcome measure was collected and scored by an independent research staff member (C.B.).
In the rest condition, participants were asked sit comfortably for 45 minutes. To control for potential deleterious effects related to boredom that might occur during 45 minutes of rest, participants completed lightly stimulating games and questionnaires. Before and after the rest condition, participants completed the POMS questionnaire.
Outcome Measure: The POMS Questionnaire
The abbreviated 30-item version of the POMS questionnaire19 has been used to examine mood states in persons with MS.11 It consists of 30 adjectives that are rated using the “right now” (eg, “fill in one circle…which best describes how you feel right now”) response set on a 5-point scale with anchors of 0 (not at all) and 4 (extremely). The “right now” response set allows for measuring the changes in mood from immediately before to after aquatic exercise, thereby isolating factors that can influence mood during the session. Several subscales can be calculated to examine Anxiety-Tension, Anger-Hostility, Depression-Dejection, Fatigue-Inertia, Vigor-Activity, and Confusion-Bewilderment. Total mood disturbance (TMD) score was calculated by summing all the scores from the subscales of Anxiety-Tension, Anger-Hostility, Depression-Dejection, Fatigue-Inertia, and Confusion-Bewilderment and then subtracting the score from the Vigor-Activity subscale. Lower TMD scores indicate better mood. Higher scores on the Vigor-Activity subscale indicate increased vigorousness. For all other subscales and TMD, higher scores indicated worse mood.
Statistical Analysis
Analyses were conducted using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp, Armonk, NY). Acute effects of aquatic exercise measured by the POMS questionnaire were analyzed using a two-way repeated-measures analysis of variance (RM-ANOVA; time × condition). We examined studentized residuals for outliers and found no residuals greater than ±3. Given the small sample size and pilot nature of the study, we interpreted the results based on effect size using partial eta-squared (ηp2) values.20 Finally, paired-samples t tests were run to confirm ANOVA findings by examining assessments of mood pre versus post each condition (aquatic exercise vs rest).
Results
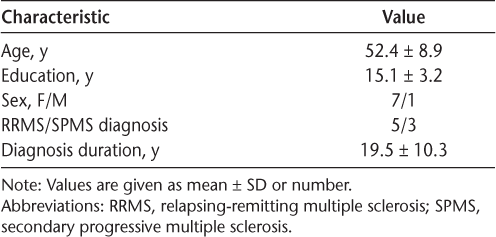
Demographic information is presented in Table 1. Eight participants were included in the study across different disease subtypes.


Participant demographic characteristics
Acute Effects of Single Bout of Aquatic Exercise on Mood
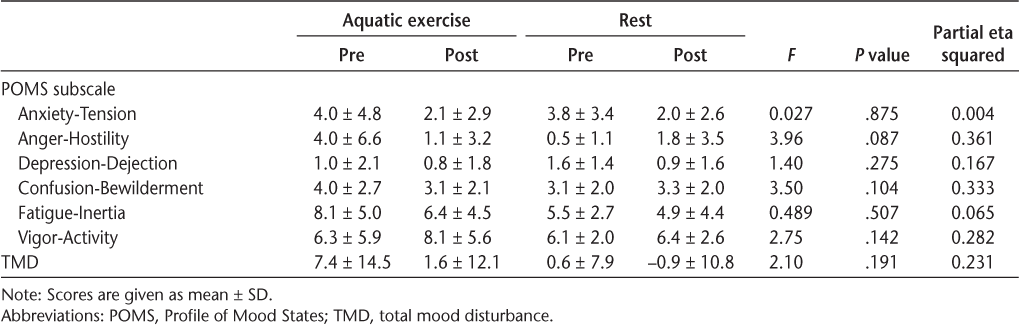
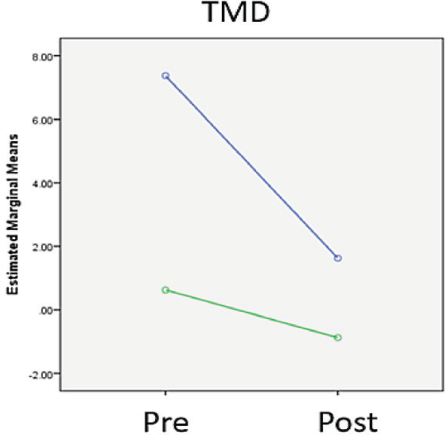
The pre-post condition mean ± SD scores for the POMS subscales are summarized in Table 2. Regarding TMD, RM-ANOVA revealed a nonsignificant interaction of time (pre vs post) × condition (aquatic exercise vs rest) in that a greater improvement in symptoms was observed immediately after the aquatic exercise condition compared with the rest condition (Figure 1). The effect size was large (ηp2 = 0.23), and the pattern of change was confirmed by a paired-samples t test, which showed a significant improvement in mood symptoms after a single bout of aquatic exercise (P = .045) compared with no significant change after the rest condition (P = .568).


POMS and TMD scores pre versus post a single bout of aquatic exercise or rest


Total mood disturbance (TMD) scores pre versus post aquatic exercise (blue) and rest (green)
Regarding Fatigue, RM-ANOVA revealed a nonsignificant interaction of time × condition in that a greater reduction of fatigue was observed after aquatic exercise compared with after rest. The effect size was medium (ηp2 = 0.07), and the pattern of change was confirmed by a paired-samples t test, which showed a significant improvement in fatigue symptoms after aquatic exercise (P = .041) compared with no significant change after a bout of rest (P = .603).
Regarding Vigor, RM-ANOVA revealed a nonsignificant interaction of time × condition in that a greater increase of vigor was observed after aquatic exercise compared with after rest. The effect size was large (ηp2 = 0.28), and the pattern of change was also observed via a paired-samples t test, which showed a marginally significant increase in vigor after aquatic exercise (P = .059) compared with no significant change after a bout of rest (P = .749).
Regarding Depression, RM-ANOVA revealed a nonsignificant interaction (time × condition) that was driven by a reduction of depressive symptoms after rest compared with after aquatic exercise, which was opposite of what was expected. This pattern was confirmed by a paired-samples t test in which depressive symptoms improved significantly after rest (P = .048) compared with after aquatic exercise (P = .170).
Regarding Anger and Confusion, RM-ANOVA revealed a nonsignificant interaction (time × condition), where anger and confusion were reduced after a single bout of aquatic exercise compared with after the rest condition, where these symptoms slightly increased. The effect sizes for Anger (ηp2 = 0.36) and Confusion (ηp2 = 0.33) were both large. However, the paired-samples t tests did not show a significant difference pre to post either condition.
Finally, regarding Tension, RM-ANOVA revealed a significant effect of time (P = .015, ηp2 = 0.594) but not a time × group interaction (ηp2 = 0.004), indicating that tension was reduced similarly under both conditions. A paired-samples t test confirmed this finding in that there was a significant change pre to post both aquatic exercise (P < .001) and rest (P = .005).
Discussion
This pilot study sought to determine the acute effects of a single bout of aquatic exercise on mood in a small sample of people with MS. The study showed that immediately after a single bout of aquatic exercise, TMD and fatigue were decreased and vigor was increased compared with after rest. This study is the first, to our knowledge, to examine the effects of a single bout of aquatic exercise on mood. Although a larger sample is needed to confirm the present findings, it seems that a single bout of aquatic exercise may be a potential method for improving acute mood symptoms in persons with MS. These findings are important in that mood disturbance is particularly elevated in individuals with MS.21,22
These findings extend a handful of studies examining the effects of acute bouts of exercise in land-based exercise conditions, including walking and yoga.9–11 Aquatic exercise may be a more appealing exercise type for some participants compared with land-based exercise. Recently, it was reported that MS alters the thermoregulatory response during exercise, making it more difficult for persons with MS to regulate their body temperature during certain types of exercise.23 Because it is performed in the water, aquatic exercise may be a more preferred exercise type for those who experience overheating. Also, some people with MS cannot participate in walking or other types of land-based exercise due to an inability to use their legs. Aquatic exercise (specifically in pools in which they can be safely transferred) enables the use of buoyancy to allow for lower extremity exercise. Future studies comparing land-based exercise with aquatic exercise may reveal what factors determine what types of exercise are best for certain people.
Interestingly, we found that tension was significantly reduced across both conditions. This finding replicates what was found by a recent study comparing a single bout of rest with two types of land-based exercise in which a main effect of time was found for tension.10 It is unclear why rest would cause a reduction in tension to the same degree as aquatic exercise. One possibility is that the participants found the rest condition relaxing in some way, perhaps because they were not required to do anything other than mildly stimulating activities.
The present study has several limitations. The statistical power of the results is limited by the small sample size. However, the results provided proof-of-concept data that can guide the development and execution of further larger trials. Another limitation involves study design. It would have been optimal to present the aquatic exercise and rest conditions in a counterbalanced order, randomized across participants. However, this study was part of a larger study examining the effects of a longer aquatic exercise program, so the rest condition was always given at baseline. Future investigations presenting the conditions in a counterbalanced manner would help verify the present findings. Finally, we examined the mood symptoms immediately after the single bout of exercise or rest, which gave us information on only the immediacy of the results. Future studies including assessment of mood symptoms for a longer period after either condition would help researchers understand how long the effects of aquatic exercise last after a single bout.
Even with these limitations, the present study is the first, to our knowledge, to investigate the effects of a single bout of aquatic exercise on mood in people with MS, showing encouraging results. The results indicate that aquatic exercise may be an effective technique for improving acute mood symptoms, similar to what has been reported for several types of land-based exercises.10,11 Although we were not able to compare the effects of land-based ET and aquatic exercise, future studies may be able to determine whether both modalities of exercise are similarly effective at managing mood symptoms. It also should be considered that persons with MS who are reluctant to perform land-based ET may find aquatic exercise more tolerable because it may help the patient avoid overheating during ET (if the temperature of the pool is properly controlled), cause less stress on joints, and help with spasticity. Further studies with large samples could help in the development of aquatic exercise programs to treat mood symptoms in people with MS.
PRACTICE POINTS
A single bout of aquatic exercise may be effective in improving acute mood symptoms in people with MS.
Fatigue reductions after a single session of aquatic exercise were observed as well.
Future studies with larger samples should be conducted to gain a better understanding of acute effects of aquatic exercise on mood.
Acknowledgments
The authors thank Ann Marie Peterson and Ellen Daudelin for their support of this project, as well as Jeffrey Zhang for assisting us with statistics.
References
Jones KH, Ford DV, Jones PA, et al. A large-scale study of anxiety and depression in people with multiple sclerosis: a survey via the web portal of the UK MS Register. PLoS One . 2012; 7: e41910.
Marrie RA, Reingold S, Cohen J, et al. The incidence and prevalence of psychiatric disorders in multiple sclerosis: a systematic review. Mult Scler . 2015; 21: 305– 317.
Ensari I, Motl RW, Pilutti LA. Exercise training improves depressive symptoms in people with multiple sclerosis: results of a meta-analysis. J Psychosom Res . 2014; 76: 465– 471.
Pilutti LA, Greenlee TA, Motl RW, Nickrent MS, Petruzzello SJ. Effects of exercise training on fatigue in multiple sclerosis: a meta-analysis. Psychosom Med . 2013; 75: 575– 580.
Latimer-Cheung AE, Martin Ginis KA, Hicks AL, et al. Development of evidence-informed physical activity guidelines for adults with multiple sclerosis. Arch Phys Med Rehabil . 2013; 94: 1829– 1836.e7.
Dalgas U, Stenager E, Sloth M. The effect of exercise on depressive symptoms in multiple sclerosis based on a meta-analysis and critical review of the literature. Eur J Neurol . 2015; 22: 443– e34.
Motl RW, Pilutti LA. The benefits of exercise training in multiple sclerosis. Nat Rev Neurol. 2012; 8: 487– 497.
Platta ME, Ensari I, Motl RW, Pilutti LA. Effect of exercise training on fitness in multiple sclerosis: a meta-analysis. Arch Phys Med Rehabil . 2016; 97: 1564– 1572.
Sandroff BM, Hillman CH, Benedict RHB, Motl RW. Acute effects of varying intensities of treadmill walking exercise on inhibitory control in persons with multiple sclerosis: a pilot investigation. Physiol Behav . 2016; 154: 20– 27.
Ensari I, Sandroff BM, Motl RW. Effects of single bouts of walking exercise and yoga on acute mood symptoms in people with multiple sclerosis. Int J MS Care . 2016; 18: 1– 8.
Ensari I, Sandroff BM, Motl RW. Intensity of treadmill walking exercise on acute mood symptoms in persons with multiple sclerosis. Anxiety Stress Coping . 2017; 30: 15– 25.
American Physical Therapy Association. Guide to physical therapist practice, part 1: a description of patient/client management, part 2: preferred practice patterns. Phys Ther . 1997; 77: 1160– 1656.
Frohman AN, Okuda DT, Beh S, et al. Aquatic training in MS: neurotherapeutic impact upon quality of life. Ann Clin Transl Neurol . 2015; 2: 864– 872.
Kargarfard M, Etemadifar M, Baker P, Mehrabi M, Hayatbakhsh R. Effect of aquatic exercise training on fatigue and health-related quality of life in patients with multiple sclerosis. Arch Phys Med Rehabil . 2012; 93: 1701– 1708.
Razazian N, Yavari Z, Farnia V, et al. Exercising impacts on fatigue, depression, and paresthesia in female patients with multiple sclerosis. Med Sci Sports Exerc . 2016; 48: 796– 803.
Aidar FJ, Gama de Matos D, de Souza RF, et al. Influence of aquatic exercises in physical condition in patients with multiple sclerosis. J Sports Med Phys Fitness . 2018; 58: 684– 689.
Castro-Sánchez AM, Matarán-Peñarrocha GA, Lara-Palomo I, Saavedra-Hernández M, Arroyo-Morales M, Moreno-Lorenzo C. Hydrotherapy for the treatment of pain in people with multiple sclerosis: a randomized controlled trial. Evid Based Complement Alternat Med . 2012; 2012: 473963.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol . 2011; 69: 292– 302.
McNair DM, Lorr M, Droppleman LF. Manual for the Profile of Mood States (POMS). San Diego, CA: Educational Industries Testing Services; 1971.
Richardson JTE. Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev . 2011; 6: 135– 147.
Feinstein A. Mood disorders in multiple sclerosis and the effects on cognition. J Neurol Sci . 2006; 245: 63– 66.
Boeschoten RE, Braamse AMJ, Beekman ATF, et al. Prevalence of depression and anxiety in multiple sclerosis: a systematic review and meta-analysis. J Neurol Sci . 2017; 372: 331– 341.
Allen DR, Huang M, Morris NB, et al. Impaired thermoregulatory function during dynamic exercise in multiple sclerosis. Med Sci Sports Exerc . 2019; 51: 395– 404.








