

Publication
Research Article
International Journal of MS Care
Disease-Modifying Therapies During the COVID-19 Outbreak
Abstract
Background:
Managing multiple sclerosis (MS) during the novel coronavirus disease 2019 (COVID-19) pandemic is a challenge due to the lack of evidence from clinical studies. Disease-modifying therapies (DMTs) may affect the immune response and subsequently alter the risk of COVID-19 infections.
Methods:
A literature search was conducted on the MEDLINE, Embase, and Cochrane databases. A focused Google search was also performed. Recommendations regarding the use of DMTs during the COVID-19 outbreak from national and international MS/neurology societies were identified and reviewed.
Results:
The review included 16 recommendations from international and national MS organizations. All recommendations are based on expert opinions. The recommendations regarding DMT initiation and management during this outbreak are summarized. Moreover, the experts’ views about the risk of COVID-19 infection with each DMT are discussed.
Conclusions:
There is significant agreement among most experts’ recommendations from a variety of sources based on collective clinical experience. However, the recommendations will likely evolve because sufficient clinical data are limited. Several ongoing registries will help provide information for future recommendations.
The novel coronavirus disease 2019 (COVID-19) is a current global challenge. In December 2019, clusters of patients with pneumonia of unknown etiology were reported in Wuhan, Hubei Province, China. By analyzing samples from the patients, a novel Betacoronavirus was discovered by the China Novel Coronavirus Investigating and Research Team.1 Subsequently, the novel coronavirus became an outbreak in many regions across the globe. On March 11, 2020, the World Health Organization declared the COVID-19 outbreak a global pandemic.2
Multiple sclerosis (MS) is the most prevalent chronic immune-mediated disorder of the central nervous system, affecting more than 2 million people worldwide.3 In the past few decades, several disease-modifying therapies (DMTs) with variable mechanisms of action were developed for the treatment of MS. The resultant modulation and suppression of the immune system by these DMTs may alter the risk of infection in patients with MS. Currently, there is no consensus guiding clinicians to manage DMTs during this pandemic.
This article includes a narrative review of the international and national recommendations regarding DMT management during the COVID-19 pandemic. Furthermore, this review discusses the immunopathogenesis of coronavirus and the effects of DMTs on the immune system.
Methods
Literature Search Strategy
Two of us (S.T. and M.A.) independently searched for publication articles indexed in the MEDLINE, Embase, and Cochrane databases from inception to April 14, 2020. A focused Google search was also completed on the same day. The search strategy included the various terms for MS and coronavirus. The search strategy is available in Table S1, which is published in the online version of this article at ijmsc.org. The reference lists of the included articles and the relevant links were also manually reviewed for additional eligible articles. Non–English language articles were reviewed by a physician who is a native speaker of or an expert in that language.
Selection Criteria and Data Extraction
The inclusion criteria for the narrative review included the recommendations regarding the use of DMTs during the COVID-19 outbreak from national and international MS/neurology societies. Data extraction was independently performed by two of us (S.T. and M.A.). A standardized data collection form was used to extract the following information: the names of MS societies, recommendations for starting and managing DMTs during the COVID-19 outbreak, risk of COVID-19 infection of each DMT, and management of DMTs in patients with active COVID-19. Any discrepancies found in the data record forms were resolved by referring to the original articles.
Results
The literature review process is shown in Figure S1. The review included 16 recommendations from international and national MS organizations, including the Multiple Sclerosis International Federation (MSIF),4 the European Academy of Neurology (EAN),5 the European Multiple Sclerosis Platform (EMSP),6 Multiple Sclerosis Australia (MSA),7 the Francophone Society of Multiple Sclerosis (SFSEP),8 the Multiple Sclerosis Society of Ireland (MSS-Ireland),9 the Italian Multiple Sclerosis Association (AISM),10 the Multiple Sclerosis Society of New Zealand (MSNZ),11 Multiple Sclerosis Spain,12 the Swiss Multiple Sclerosis Society (Swiss MSS),13 the Association of British Neurologists (ABN),14 the Multiple Sclerosis Society of the United Kingdom (MSS-UK),15 and the National Multiple Sclerosis Society (NMSS) of the United States. The MSIF and EMSP recommendations are the same. Several national societies, including the Brazilian Multiple Sclerosis Association,16 The Japanese Society of Neuroimmunology,17 and Stichting MS Research,18 have translated the MSIF recommendations into their respective languages. All recommendations are based on expert opinions. The summary of the recommendations is shown in Table 1.


Summary of recommendations regarding use of disease-modifying therapies during COVID-19 outbreak
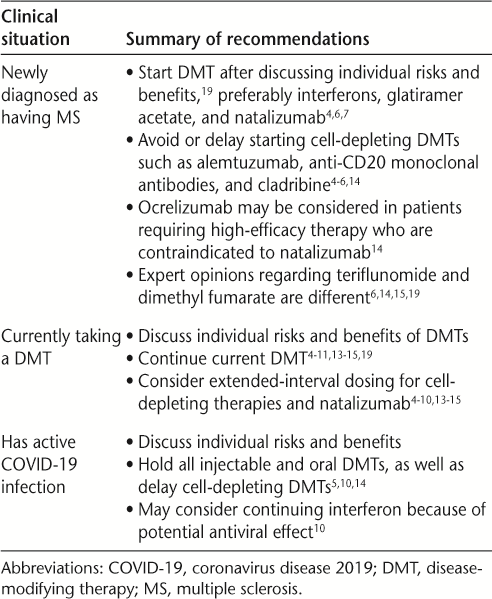
Starting DMTs
The NMSS recommends starting a DMT in patients with a recent diagnosis of MS. Both MS providers and patients with MS should discuss the risk of infection, including COVID-19, weighing against MS activity, age, other medical conditions, and other potential factors that could affect DMT.19 The risk of COVID-19 in the specific region should be taken into consideration when choosing a DMT.4,6
The DMTs not associated with significant lymphopenias, such as interferons, glatiramer acetate, and natalizumab, are the preferred choices.4,6,7 The NMSS warned to consider specific risks and benefits before starting natalizumab and fingolimod because they potentially lead to an increase in disability after discontinuation.19 During the pandemic, the MSIF and the EMSP recommend careful consideration before starting teriflunomide, dimethyl fumarate, fingolimod, and siponimod.4,6 The ABN considers teriflunomide and dimethyl fumarate to be safe options to start as well.14 The MSS-UK recommends considering alternative DMTs in patients who plan to start fingolimod.15
Cell-depleting DMTs, including alemtuzumab, anti-CD20 monoclonal antibodies, and cladribine, are not considered favorable options given the prolonged effect on lymphopenia.4,6 The EAN advises considering delayed initiation of these DMTs until the peak of the pandemic is over in the region, except when the benefit of therapy outweighs the risk of severe COVID-19 infection.5 According to the ABN recommendation, alemtuzumab and cladribine should not be started during the pandemic. Although the persistently higher risk of infection is anticipated during the virus outbreak, ocrelizumab may be an option if a high-efficacy DMT is indicated and a patient is not eligible for natalizumab.14
Continuation of DMTs
All patients with MS without an active infection should continue with their current DMT, especially interferons, glatiramer acetate, teriflunomide, dimethyl fumarate, fingolimod, and natalizumab.4–11,13–15,19 Although the ABN considers natalizumab to be a safe option, considering extended-interval dosing may be appropriate.14 Most of the MS organizations recommend considering delaying dosing for cell-depleting therapies based on individual risk of relapse and infection.4–10,13–15 For infusion therapies, the EAN advises considering infusion at home rather than at an infusion center depending on the regional COVID-19 incidence.5 In addition, the EAN, MSA, and MSNZ recommend continuing intermittent immunotherapies (ie, plasma exchange and intravenous immunoglobulin) with an appropriate preventive measure of COVID-19 infection.5,7,11
The MSNZ advises keeping blood monitoring for DMTs up to date in patients taking teriflunomide, dimethyl fumarate, fingolimod, siponimod, or natalizumab. If lymphopenia occurs, frequent monitoring may be needed.11 Because of increasing pressures on health care services and the elevated risk of infection in patients visiting clinics or hospitals, blood monitoring may need to be abbreviated in some situations. The ABN proposed minimal blood monitoring during this outbreak. However, patients must remain vigilant to recognize signs or symptoms of adverse events to medications.14
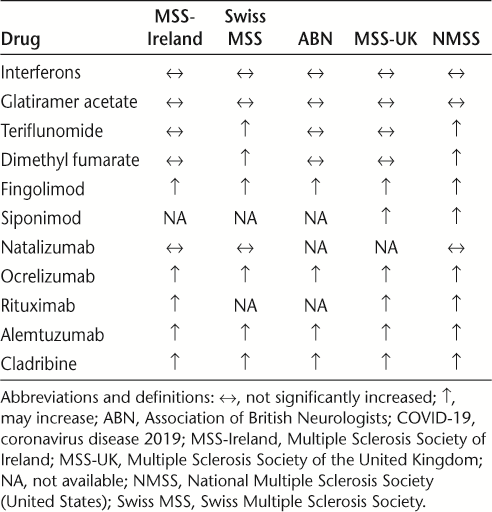
Risk of COVID-19 Infection in Patients on DMT
Currently there is no clinical study to determine the risk of coronavirus infection in patients with MS. The NMSS, MSS-UK, ABN, MSS-Ireland, and Swiss MSS have provided opinions regarding the risk of COVID-19 infection. Interferons,7,13–15,19 glatiramer acetate,7,9,13,15,19 and natalizumab9,13,19 are not considered to significantly elevate the risk. There is a significant concern of increased COVID-19 infection risk with alemtuzumab, anti-CD20 monoclonal antibodies, and cladribine.9,13–15,19 Some concerns are raised with fingolimod5,9,13–15,19 and siponimod5,15,19 as well. Although the MSS-UK and MSS-Ireland do not consider an increased risk in patients with teriflunomide and dimethyl fumarate, the NMSS and the Swiss MSS have a concern that these DMTs may elevate the risk. The expert opinions regarding the risk of COVID-19 infection and DMTs are summarized in Table 2.


Expert opinions regarding risk of COVID-19 infection in patients receiving disease-modifying therapies
Management of DMTs During Active COVID-19 Infection
The EAN, AISM, and ABN recommend holding all injectable and oral DMTs and delaying cell-depleting DMTs.5,10,14 However, physicians may consider continuing interferon because of the potential antiviral effect.10 For patients taking fingolimod and natalizumab, there is a concern about rebound disease activity after discontinuation. Physicians must individualize the treatment plans based on the clinical situation.
Hematopoietic Stem Cell Therapy
Hematopoietic stem cell therapy includes intense chemotherapy; therefore, it severely impairs the immune response for an extended interval. All experts recommend considering postponing the procedure.4,6,7,9,14,15 Furthermore, the patients who underwent recent hematopoietic stem cell therapy should extend the isolation period.4,6,7
Discussion
Currently there are no data from observational studies or clinical trials guiding health care providers to manage DMTs for MS during the current COVID-19 pandemic. All recommendations from international and national MS societies are based on expert opinions. There was no major disagreement among experts’ views. However, the recommendations from each organization may change as the situation evolves. We encourage practitioners to visit the websites provided in Table S2 for the latest information.
It is also important to understand the effect of COVID-19 on the immune system to understand these latest recommendations. There are currently seven known strains of coronavirus that infect humans (HCoVs): 229E, OC43, HKU1, and NL63 are community-acquired strains and cause the common cold, whereas the 2003 severe acute respiratory syndrome CoV (SARS-CoV) and the 2012 Middle East respiratory syndrome CoV (MERS-CoV) caused severe respiratory illnesses.20–22 The newest HCoV, SARS-CoV-2 (also known as 2019nCoV, and previously named Wuhan coronavirus), is the cause of the current COVID-19 pandemic.
In most cases of COVID-19 infection, the individuals developed lymphopenia.23 Severe cases requiring intensive care unit admittance had high levels of proinflammatory cytokines, such as interleukins 2, 7, and 10, as well as granulocyte colony-stimulating factor and tumor necrosis factor alpha.23 A recent cohort has shown that neutrophilia, lymphopenia, and decreased CD3 and CD4 counts are associated with higher risks of the development of acute respiratory distress syndrome (ARDS).24
Further pathogenesis has been challenging to determine because of the novelty of this virus; however, SARS-CoV-2 is from the same lineage as SARS-CoV and shares 82% of its genetic material, and, indeed, the pathogenesis is quite similar between the two viruses.25,26 It is, therefore, fair to deduce further information about SARS-CoV-2 based on what we know from SARS-CoV. It is known that SARS-CoV has at least seven interferon antagonists.27 In an animal study, rapid SARS-CoV replication induced a delayed interferon alfa and interferon beta (IFNβ) response, which is an essential response to viral infection.28 A study from 128 SARS-CoV convalescent samples demonstrated the importance of adaptive immunity, especially CD8+ T-cell response. Moreover, most of the SARS-CoV convalescent possessed a strong neutralizing antibody produced by B cells.29
Generally, DMTs for MS involve some form of immunomodulation, immune cell sequestration, or immunosuppression. Therefore, DMTs may alter the risk of COVID-19 infection and the disease course during this pandemic. Several DMTs, especially cell-depleting DMTs, can cause lymphopenia, which is associated with adverse outcomes in COVID-19 infection.24
As the oldest MS DMT, IFNβ now exists in several formulations, including IFNβ-1a, IFNβ-1b, and PEG-IFNβ-1a; IFNβ is believed to downregulate proinflammatory cytokine production as well as decrease T-cell activation and migration.30 Although lymphopenia is common, the events are mild and transient.31 Data from clinical trials and more than 20 years of real-life experience have not revealed an increased prevalence of specific infections except for local infection at the injection site.30 In a physiologic state, IFNα and IFNβ signaling pathways play a role in the defense against viral infection. Moreover, an in vitro study demonstrated a capacity of cytopathic effect inhibition of IFNβ-1b in SARS-CoV–infected cells.32 Experts’ opinions from all national MS and neurology societies indicate a belief that interferons will not increase the risk of COVID-19 infection.9,13–15,19 Furthermore, IFNβ, combined with lopinavir/ritonavir and ribavirin, is currently in a clinical trial for the treatment of COVID-19 (www.clinicaltrials.gov; identifier: NCT04276688).
The proposed mechanism of glatiramer acetate is promoting the development of regulatory T-helper 2 cells, which decrease the inflammatory response.33 Leukopenia is uncommon in patients with glatiramer acetate. When it occurs, it is generally mild.34 Not surprisingly, current expert opinions agree that glatiramer acetate should not significantly elevate the risk of COVID-19 infection.9,13,15,19
Teriflunomide is an oral DMT. The proposed mechanism of action is selective and reversible inhibition of dihydroorotate dehydrogenase, a key enzyme in the de novo pyrimidine synthesis. Therefore, it leads to a reduction in the proliferation of activated T and B lymphocytes without causing cell death.35 In a phase 3 randomized controlled trial, reversible neutropenia and lymphopenia were observed in the teriflunomide group, and all patients are asymptomatic. There was no significant difference in the incidence of respiratory tract infection between the treatment and placebo groups.36 However, some minor differences exist among some experts’ opinions in the field regarding the risk of COVID-19 infection in patients taking teriflunomide.9,13,15,19
The precise mechanism of action of dimethyl fumarate is unclear. It is believed to activate nuclear factor erythroid-derived 2–related factor 2, a transcription factor. Dimethyl fumarate decreases absolute lymphocyte counts and alters the proportion of lymphocyte subsets toward an anti-inflammatory state. Reduction of CD8+ T lymphocytes was more marked than that of other lymphocyte subsets in patients with MS treated with dimethyl fumarate.37 An integrated analysis of phase 2b/3/long-term extension studies showed that the mean total lymphocyte count decreased by 30% during the first year of dimethyl fumarate therapy and subsequently stabilized.38 However, the incidences of infection in the treatment and placebo groups were not significantly different, even when stratified by total lymphocyte counts or T-cell subset frequency.37,39 Similar to teriflunomide, only minor differences exist between experts regarding the risk of COVID-19 infection in patients taking dimethyl fumarate.9,13,15,19
Fingolimod and siponimod bind to sphingosine-1 phosphate receptors on T cells, preventing lymphocyte egression from the lymph nodes into the circulation and leading to sequestration of T cells in lymph nodes. After 1 month of fingolimod therapy, circulating lymphocyte counts were reduced significantly.40 A subsequent study demonstrated the redistribution of lymphocyte subsets: increased natural killer cells and decreased CD4+ T lymphocytes.41 An integrated analysis of long-term data from phase 2/3 studies did not show a significant difference in the incidences of infections between the fingolimod and placebo groups.42 In a phase 3 study, 1% of patients treated with siponimod developed lymphopenia. The adverse events related to infection were similar in the siponimod and placebo groups except for herpes zoster reactivation (2% in siponimod, 1% in placebo).43 However, experts from national MS societies have raised concern that fingolimod9,13–15,19 and siponimod15,19 may elevate the risk of COVID-19 infection. On the other hand, there is an ongoing phase 2 clinical trial evaluating fingolimod for the prevention of ARDS in COVID-19 infection (www.clinicaltrials.gov; identifier: NCT04280588).
Natalizumab reduced the migration of leukocytes from the blood to the central nervous system by disrupting the interaction between α4 integrins and vascular cell adhesion molecule 1. As a result, circulating T and B lymphocyte levels are increased.44 In a phase 3 clinical trial, the overall incidence of infection was not different between the treatment and placebo groups. Serious infections, including severe pneumonia and urosepsis, were reported in 3.2% of patients taking natalizumab and 2.6% taking placebo.45 However, experts agree that natalizumab should not significantly increase the risk of COVID-19 infection.9,13,19 Furthermore, the ABN views natalizumab as a safe option for high-efficacy therapy during the COVID-19 pandemic.14
Ocrelizumab and rituximab are monoclonal antibodies that deplete CD20+ B lymphocytes. Ocrelizumab has been approved by the US Food and Drug Administration for both relapsing-remitting and primary progressive MS. On the other hand, rituximab is currently used off-label in various immune-mediated neurologic disorders, including MS. The median time to B-lymphocyte replenishment for ocrelizumab is 72 weeks.46 In rituximab, B-lymphocyte repopulation has considerable intraindividual variation, with the lowest and average intervals being 3.6 and 8.3 months, respectively.47 Because of the prolonged B-lymphocyte depletion, all expert panels are concerned about the increased risk of infection with both ocrelizumab9,13–15,19 and rituximab15,19 during this outbreak.
Alemtuzumab depletes circulating CD52+ lymphocytes and has reprogramming effects on tolerogenic networks of the immune system. CD8+ T-lymphocyte and B-lymphocyte restorations take approximately 3 and 6 months, respectively. Repopulation of CD4+ may take up to 1 to 2 years.48 A pooled analysis of 6-year data from three randomized trials showed that the overall infection risk with alemtuzumab decreases over time. However, lymphocyte count after alemtuzumab cannot predict the risk.49 Similar to B-cell–depleting therapies, experts agree that alemtuzumab is concerning regarding increased risk of COVID-19 infection because of its immunosuppressive effect during the first months after infusion.9,13–15,19
Cladribine is a deoxyadenosine analogue prodrug. After it is taken up by cells, it is phosphorylated to an active form, which causes DNA strand breakage, leading to cell death. Cladribine reduces total lymphocyte counts. The depletion of B lymphocytes is markedly more than that of T lymphocytes. After discontinuation of cladribine, 75% of patients have normal lymphocyte counts at week 144.50 Thus, there is a concern of increased infection risk with cladribine, at least during periods of lymphopenia, during this pandemic.9,13–15,19
Currently there are several ongoing registries collecting COVID-19 infection data in patients with MS, such as COViMS-19 (COVID-19 Infections in MS & Related Diseases; https://www.covims.org/) in North America and MuSC-19 (Multiple Sclerosis and COVID19; https://musc-19.dibris.unige.it/) in Italy. In addition, data from registries for all patients with COVID-19, such as LEOSS (Lean European Open Survey on SARS-CoV-2; https://leoss.net/), will allow researchers to compare COVID-19 infection rates between patients with MS and other populations. We encourage clinicians to share data with these registries because these databases will be invaluable resources for the development of further recommendations.
Conclusion
Despite a lack of clinical studies, several international and national MS societies have provided expert opinions regarding DMT management during the current COVID-19 outbreak. There was no major disagreement among expert views. Notably, several DMTs can cause lymphopenia, and a recent cohort study showed that lymphopenia is a risk factor for ARDS in COVID-19 infection. Understanding the immunopathogenesis of coronavirus infection, as well as the DMTs’ mechanisms of action and their effects on the immune system, will assist in clinical decision making. Data from the current ongoing registries will provide evidence for future recommendations.
PRACTICE POINTS
There are no clinical trials or observational studies guiding treatment decisions for MS in the current coronavirus disease 2019 (COVID-19) pandemic. Recommendations are from expert opinions. Therefore, treatment should be tailored to an individual after a detailed discussion of risks and benefits.
Disease-modifying therapies (DMTs) that do not decrease lymphocyte counts are the preferred options for starting MS treatment during the COVID-19 outbreak.
Patients who are currently taking a DMT should continue the treatment. Extended-interval dosing for cell-depleting therapies and natalizumab may be considered.
In patients with active COVID-19 infection, a clinician may consider holding all injectable and oral DMTs, as well as delaying cell-depleting DMTs.
Financial Disclosures
Dr Avila is a consultant and speaker for educational programs for Genzyme, Genentech, Novartis, and Alexion. The other authors declare no conflicts of interest.
References
Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020; 382: 727– 733.
World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020. Published March 11, 2020. Accessed March 19, 2020.
Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019; 18: 459– 480.
Multiple Sclerosis International Federation. The coronavirus and MS – global advice. https://www.msif.org/news/2020/02/10/the-coronavirus-and-ms-what-you-need-to-know/. Published 2020. Updated March 18, 2020. Accessed April 14, 2020.
Filippi M, Hochmeister S, Oreja-Guevara C, Tanasescu R, Wiendl H. Immunotherapy for patients with neuroimmunological disorders during the COVID-19 pandemic. https://www.ean.org/fileadmin/user_upload/ean/ean/EANcore_COVID-19/recommendations___guidelines/Guidelines_for_neurological_disorders_immuntherapy_and_COVID19_final.pdf. Published March 24, 2020. Accessed April 14, 2020.
European Multiple Sclerosis Platform. Coronavirus disease (COVID-19) and MS. http://www.emsp.org/news-messages/coronavirus-disease-covid-19-and-multiple-sclerosis/. Published 2020. Accessed April 14, 2020.
Multiple Sclerosis Australia. COVID-19 information for people with MS. https://www.msaustralia.org.au/about-ms/covid-19-information-people-ms. Published 2020. Last updated April 5, 2020. Accessed April 14, 2020.
Conseil Médico-Scientifique (CMS), Comité Inter-Régional Médical de l’ARSEP (CIRMA) de la Fondation ARSEP, Centres de Ressource et de Compétence SEP (CRC-SEP), Conseil d’Administration de la Société Francophone de la SEP (SF-SEP), Ligue Française contre la SEP (LFSEP), Centre de Référence des Maladies Inflammatoires Rares du Cerveau Et de la Moelle (MIRCEM). General instructions to limit the risks of contagion by the COVID-19 virus in people with MS, NMO or other demyelinating pathologies at risk of severe infection. https://sfsep.org/conseils-a-propos-du-covid-19-pour-les-personnes-atteintes-de-sep/. Published 2020. Accessed April 14, 2020.
Multiple Sclerosis Society of Ireland. COVID-19 and MS. https://www.ms-society.ie/covid-19-and-ms. Published 2020. Accessed April 14, 2020.
Associazione Italiana Sclerosi Multipla. Information on the management of the patient with MS during the epidemic of COVID-19 https://www.aism.it/sites/default/files/ComunicazioneGdSSINSM-Coronavirus.pdf. Published 2020. Accessed April 14, 2020.
Mason D, Boggild M, van der Walt HB, et al. [Updated] COVID-19 – advice for patients. https://www.msnz.org.nz/covid-19-advice-for-patients/. Published April 9, 2020. Accessed April 14, 2020.
Esclerosis Múltiple España. Recommendations on the coronavirus COVID-19 for people with multiple sclerosis. https://www.esclerosis-multiple.com/el-coronavirus-y-la-esclerosis-multiple-lo-que-necesita-saber/. Published 2020. Accessed April 14, 2020.
Swiss Multiple Sclerosis Society. MS and COVID-19: recommendations for Switzerland. https://www.multiplesklerose.ch/de/aktuelles/detail/ms-und-covid-19-empfehlungen-fuer-die-schweiz/#a_genauere-ausfuehrungen-zu-ms-medikamenten. Published 2020. Updated March 17, 2020. Accessed April 14, 2020.
Coles A, Lim M, Giovannoni G, Anderson P, Dorsey-Campbell R, Qualie M. ABN guidance on the use of disease-modifying therapies in multiple sclerosis in response to the threat of a coronavirus epidemic. https://cdn.ymaws.com/www.theabn.org/resource/collection/65C334C7-30FA-45DB-93AA-74B3A3A20293/02.04.20_ABN_Guidance_on_DMTs_for_MS_and_COVID19_VERSION_4_April_2nd.pdf. Published 2020. Accessed April 14, 2020.
Multiple Sclerosis Society. COVID-19 coronavirus and MS treatments. https://www.mssociety.org.uk/about-ms/treatments-and-therapies/disease-modifying-therapies/covid-19-coronavirus-and-ms. Published 2020. Accessed April 14, 2020.
Brazilian Multiple Sclerosis Association. COVID-19 global advice for people with MS. http://abem.org.br/27253-2/?fbclid=IwAR2NCBfORBy1sy9D-WgcXV44Y4zxUWYaZy4Fv98ZvL4og5t2lOVFrg53dxo. Published 2020. Accessed April 14, 2020.
Miyazaki Y. Multiple Sclerosis United Nations (MSIF) announces “advice for multiple sclerosis patients about new coronavirus.” http://www.neuroimmunology.jp/jpn/news/COVID19_20200315.pdf. Published 2020. Accessed April 14, 2020.
Stichting MS Research. Worldwide COVID-19 advice for people with MS. https://msresearch.nl/wereldwijd-covid-19-advies-voor-mensen-met-ms?utm_source=Aanmelding+nieuwsbrief+MS+Research&utm_campaign=acf90a9f4c-EMAIL_CAMPAIGN_2020_03_16_09_24&utm_medium=email&utm_term=0_ec75ab155f-acf90a9f4c-147715973. Published 2020. Accessed April 14, 2020.
National Multiple Sclerosis Society. Disease modifying therapies during the COVID-19 pandemic. https://www.nationalmssociety.org/What-you-need-to-know-about-Coronavirus-(COVID-19)/DMT-Guidelines-for-Coronavirus-(COVID-19)-and. Published 2020. Accessed April 14, 2020.
McIntosh K, Chao RK, Krause HE, Wasil R, Mocega HE, Mufson MA. Coronavirus infection in acute lower respiratory tract disease of infants. J Infect Dis. 1974; 130: 502– 507.
Peiris JS, Lai ST, Poon LL, et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. 2003; 361: 1319– 1325.
Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012; 367: 1814– 1820.
Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395: 497– 506.
Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China [published online ahead of print March 13, 2020]. JAMA Intern Med. doi: 10.1001/jamainternmed.2020.0994.
Chan JF, Kok KH, Zhu Z, et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect. 2020; 9: 221– 236.
Fung SY, Yuen KS, Ye ZW, Chan CP, Jin DY. A tug-of-war between severe acute respiratory syndrome coronavirus 2 and host antiviral defence: lessons from other pathogenic viruses. Emerg Microbes Infect. 2020; 9: 558– 570.
Wong LY, Lui PY, Jin DY. A molecular arms race between host innate antiviral response and emerging human coronaviruses. Virol Sin. 2016; 31: 12– 23.
Channappanavar R, Fehr AR, Vijay R, et al. Dysregulated type I interferon and inflammatory monocyte-macrophage responses cause lethal pneumonia in SARS-CoV-infected mice. Cell Host Microbe. 2016; 19: 181– 193.
Li CK, Wu H, Yan H, et al. T cell responses to whole SARS coronavirus in humans. J Immunol. 2008; 181: 5490– 5500.
Winkelmann A, Loebermann M, Reisinger EC, Hartung HP, Zettl UK. Disease-modifying therapies and infectious risks in multiple sclerosis. Nat Rev Neurol. 2016; 12: 217– 233.
Rieckmann P, O’Connor P, Francis GS, Wetherill G, Alteri E. Haematological effects of interferon-beta-1a (Rebif) therapy in multiple sclerosis. Drug Saf. 2004; 27: 745– 756.
Tan EL, Ooi EE, Lin CY, et al. Inhibition of SARS coronavirus infection in vitro with clinically approved antiviral drugs. Emerg Infect Dis. 2004; 10: 581– 586.
Weber MS, Hohlfeld R, Zamvil SS. Mechanism of action of glatiramer acetate in treatment of multiple sclerosis. Neurotherapeutics. 2007; 4: 647– 653.
Fox EJ, Buckle GJ, Singer B, Singh V, Boster A. Lymphopenia and DMTs for relapsing forms of MS. Neurology Clin Pract. 2019; 9: 53– 63.
Bar-Or A, Pachner A, Menguy-Vacheron F, Kaplan J, Wiendl H. Teriflunomide and its mechanism of action in multiple sclerosis. Drugs. 2014; 74: 659– 674.
Confavreux C, O’Connor P, Comi G, et al. Oral teriflunomide for patients with relapsing multiple sclerosis (TOWER): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2014; 13: 247– 256.
Berkovich R, Weiner LP. Effects of dimethyl fumarate on lymphocyte subsets. Mult Scler Relat Disord. 2015; 4: 339– 341.
Fox RJ, Chan A, Gold R, et al. Characterizing absolute lymphocyte count profiles in dimethyl fumarate-treated patients with MS: patient management considerations. Neurol Clin Pract. 2016; 6: 220– 229.
Gold R, Kappos L, Arnold DL, et al. Placebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosis. N Engl J Med. 2012; 367: 1098– 1107.
Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010; 362: 402– 415.
Rudnicka J, Czerwiec M, Grywalska E, et al. Influence of fingolimod on basic lymphocyte subsets frequencies in the peripheral blood of multiple sclerosis patients - preliminary study. Cent Eur J Immunol. 2015; 40: 354– 359.
Kappos L, Cohen J, Collins W, et al. Fingolimod in relapsing multiple sclerosis: an integrated analysis of safety findings. Mult Scler Relat Disord. 2014; 3: 494– 504.
Kappos L, Bar-Or A, Cree BAC, et al. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet. 2018; 391: 1263– 1273.
Koudriavtseva T, Sbardella E, Trento E, Bordignon V, D’Agosto G, Cordiali-Fei P. Long-term follow-up of peripheral lymphocyte subsets in a cohort of multiple sclerosis patients treated with natalizumab. Clin Exp Immunol. 2014; 176: 320– 326.
Polman CH, O’Connor PW, Havrdova E, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006; 354: 899– 910.
Mulero P, Midaglia L, Montalban X. Ocrelizumab: a new milestone in multiple sclerosis therapy. Ther Adv Neurol Disord. 2018; 11: 1756286418773025.
Ellwardt E, Ellwardt L, Bittner S, Zipp F. Monitoring B-cell repopulation after depletion therapy in neurologic patients. Neurol Neuroimmunol Neuroinflamm. 2018; 5: e463.
Zhang X, Tao Y, Chopra M, et al. Differential reconstitution of T cell subsets following immunodepleting treatment with alemtuzumab (anti-CD52 monoclonal antibody) in patients with relapsing-remitting multiple sclerosis. J Immunol. 2013; 191: 5867– 5874.
Wray S, Havrdova E, Snydman DR, et al. Infection risk with alemtuzumab decreases over time: pooled analysis of 6-year data from the CAMMS223, CARE-MS I, and CARE-MS II studies and the CAMMS03409 extension study. Mult Scler. 2019; 25: 1605– 1617.
Deeks ED. Cladribine tablets: a review in relapsing MS. CNS Drugs. 2018; 32: 785– 796.
Supplementary Material








