Practice Points
- Ocean sailing is a feasible and safe activity for people with multiple sclerosis.
- Ocean sailing is a novel, experience-based approach to rehabilitation outside traditional clinical settings.


Publication
Research Article
Activity Available Online: To access the article and evaluation online, go to https://www.highmarksce.com/mscare.
Target Audience: The target audience for this activity is physicians, advanced practice clinicians, nursing professionals, rehabilitation professionals, social workers, and other health care providers involved in the care of people with multiple sclerosis (MS).
Learning Objectives:
Accreditation: In support of improving patient care, this activity has been planned and implemented by the Consortium of Multiple Sclerosis Centers (CMSC) and Intellisphere, LLC. The CMSC is jointly accredited by the Accreditation Council for Continuing Medical Education, the Accreditation Council for Pharmacy Education, and the American Nurses Credentialing Center, to provide continuing education for the health care team.
This activity was planned by and for the health care team, and learners will receive 0.75 Interprofessional Continuing Education credit for learning and change.
Physicians: The CMSC designates this journal-based activity for a maximum of 0.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nurses: The CMSC designates this enduring material for 0.75 contact hour of nursing continuing professional development (none in the area of pharmacology).
Psychologists: This activity is awarded 0.75 CE credits.
Social Workers: As a jointly accredited organization, the CMSC is approved to offer social work continuing education by the Association of Social Work Boards Approved Continuing Education program. Organizations, not individual courses, are approved under this program. Regulatory boards are the final authority on courses accepted for continuing education credit. Social workers completing this course receive 0.75 general continuing education credits.
Disclosures: It is the policy of the CMSC to mitigate all relevant financial disclosures from planners, faculty, and other persons that can affect the content of this CE activity. For this activity, all relevant disclosures have been mitigated. Francois Bethoux, MD, editor in chief of the International Journal of MS Care (IJMSC), has served as physician planner for this activity. He has disclosed no relevant financial relationships. Alissa Mary Willis, MD, associate editor of IJMSC, has disclosed no relevant financial relationships. Elizabeth S. Gromisch, PhD, associate editor of IJMSC, has disclosed no relevant financial relationships. Authors Jon Skovgaard Jensen, MSc; Anders Kløve Petz, MSc; Trine Nielsen, MD; Lasse Jager Pedersen, MSc; Emil Gutfelt Overgaard, MSc; Morten Blinkenberg, MD, PhD; Ulrik Dalgas, PhD; Per Aagaard, PhD; Mikkel Anthonisen, MD; and Jens Bojsen-Møller, PhD, have disclosed no relevant financial relationships.
The staff at IJMSC, CMSC, and Intellisphere who are in a position to influence content have disclosed no relevant financial relationships. Laurie Scudder, DNP, NP, CMSC continuing education director, has served as a planner and reviewer for this activity. She has disclosed no relevant financial relationships.
Method of Participation:
Release date: February 23, 2026. Valid for credit through: February 23, 2028.
To receive CE credit, participants must:
Statements of Credit are awarded upon successful completion of the evaluation. There is no fee to participate in this activity.
Disclosure of Unlabeled Use: This educational activity may contain discussion of published and/or investigational uses of agents that are not approved by the US Food and Drug Administration. The CMSC and Intellisphere do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the CMSC or Intellisphere.
Disclaimer: Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any medications, diagnostic procedures, or treatments discussed in this publication should not be used by clinicians or other health care professionals without first evaluating their patients’ conditions, considering possible contraindications or risks, reviewing any applicable manufacturer’s product information, and comparing any therapeutic approach with the recommendations of other authorities.
Background: Oceans of Hope is an initiative enabling people with multiple sclerosis (MS) to participate in ocean sailing. Long-term ocean sailing has been hypothesized to promote physical performance and cognitive function in people with MS. However, the effects and feasibility of ocean sailing for rehabilitation purposes remain unexplored. The aim of this study was to evaluate the feasibility of ocean sailing to improve mechanical muscle function, physical capacity, and fine motor control in people with MS.
Methods: In this exploratory study, 15 people with MS participated in 10 days of ocean sailing. Mechanical muscle function, gait speed, postural balance, and fine motor control were tested before and after the intervention. No control group was included. Feasibility was evaluated using adverse events, serious adverse events, drop-outs, and adherence.
Results: No serious adverse events were reported, but 10 participants experienced mild or moderate seasickness. Adherence was excellent. Manual dexterity improved, and body weight was reduced after the intervention (P< .05). No other statistically significant pre- to postintervention changes were found.
Conclusions: Ocean sailing for 10 days is feasible in people with MS, as none of the participants reported serious adverse events, and seasickness was the only adverse event. No deteriorations were observed in physical or cognitive function. Thus, initial evidence suggests ocean sailing may represent a feasible and safe form of physical activity for people with MS.
From the Research Unit of Muscle Physiology and Biomechanics, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark (JSJ, AKP, LJP, EGO, PA, JB-M); Research Unit of Neurology, Department of Regional Health Research, University of Southern Denmark, Aabenraa, Denmark (TN); Danish Multiple Sclerosis Center, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark (MB); Department of Sport Science, University of Aarhus, Aarhus, Denmark (UD); Oceans of Hope Research Unit, Copenhagen, Denmark (MA). Correspondence: Jon Skovgaard Jensen, Moseskovvej 39, Odense, Denmark; email: jskovgaard@health.sdu.dk.
Multiple sclerosis (MS) is a chronic inflammatory and neurodegenerative disorder that affects the central nervous system, resulting in a progressive loss of motor, sensory, and cognitive function.1 A sailboat circumnavigation initiative was conducted in 2014-2015 (ie, Oceans of Hope, Around the World, Back to Life)2 to promote health and quality of life for people with MS. Approximately 100 people with MS from 16 countries embarked on offshore sailing journeys that lasted from 2 to 8 weeks. A study later analyzed personal reports that underscored positive effects of ocean sailing for people with MS, such as increased self-confidence, concurrent quality of life, and decreased symptoms of depression, anxiety, and stress.3 Participants had subjective perceptions of increased levels of physical well-being after weeks of sailing. However, no objective data on physical function were available to support this. Hypothetically, neuromuscular training effects may be elicited through sustained exposure to an unstable environment (ie, continuous perturbations in posture) during sailing, potentially evoking adaptive gains in lower-limb muscle strength, neuromuscular activation, and postural balance.
It is well known that exercise and physical training can have beneficial effects for people with MS.4–6 Conventional training activities for people with MS are usually effective, and typically consist of 2 to 3 training sessions of 30 to 60 minutes each per week.7 Speculatively, however, exercise interventions of longer duration, which can enable greater training volume combined with low loading intensities, may be even more beneficial and/or easier to tolerate for people with MS due to the lower intensity of exercise and the potential avoidance of exercise-induced heat sensitivity.8
Although the physical strain of ocean sailing has not been thoroughly investigated, previous studies have reported relatively high metabolic demands during long-term (weeks of) ocean sailing or racing on offshore sailing yachts (typically 50-100 feet in length) along with high demands on muscle strength and physical fitness during small-boat sail racing (Olympic class racing dinghies, eg, 49er, 49erFX, Nacra 17, and 470 crew).9,10 Although boat handling primarily consists of strength-dominant muscle activity, postural balance is chronically challenged at sea, and even off-watch activities require a continuous demand for postural balance. Perception of joint position (proprioception) and anticipation of and reaction to constant external perturbations related to waves and ship movements likely impose a challenge to the central nervous system (CNS) through the constant stream of afferent input from the peripheral nervous system (PNS), along with a sustained efferent motor output. Sailing could thus be seen as a high volume, low-intensity training modality, which may potentially have beneficial adaptive effects for people with MS. Rehabilitation through sailing has only rarely been studied in people with neurological disorders, and the physical strain of sailing has not been quantified in people with MS. Previous studies have investigated simulated sailing based on a virtual reality methodology, and found that a sailing intervention is indeed feasible and expedient in people with spinal cord injuries.11,12 Although previous activities with Oceans of Hope have shown that long-term ocean sailing is technically feasible in people with MS, there is a lack of empirical evidence to support this, as no formal assessment of safety and efficacy has yet been performed.
The present study aimed to explore the effect of ocean sailing on mechanical lower-limb muscle function, functional performance, cognitive capacity, and postural balance in people with MS and to evaluate the feasibility of ocean sailing as an intervention for people with MS.
Study Design
In this exploratory study, 15 people with MS (5 men, 10 women) volunteered to participate in a continuous 10-day ocean sailing intervention. Participants underwent a protocol of neuromuscular and biomechanical assessments 1 to 3 days prior to departure (PRE), which were repeated within 2 to 3 days of their return (POST). The sailing intervention was carried out in 3 separate rounds due to limited space on the vessel. A 3-month follow-up assessment was conducted for the first 2 groups of participants (n = 8) using the same measurement methods as described for PRE and POST.
Participants
Participants were recruited from among people with MS who took part in a 4-week summer expedition on board the Oceans of Hope 67-ft sailboat; however, participation in the summer expedition was not required for participation in the current study. The study inclusion criteria were as follows: no relapses in the previous 6 months, Expanded Disability Status Scale (EDSS) score between 2.5 and 5.5, no alterations in medication in the previous 8 weeks, cognitively able to fill out the questionnaires, functionally independent in activities of daily living, ability to swim 300 meters, and no prior experience with ocean sailing. Study participants were provided with verbal and written information about the study and submitted their written informed consent prior to inclusion. The study was approved by the National Committees on Health Research Ethics in Denmark (S-1904818) and was conducted in accordance with the World Medical Association Declaration of Helsinki. Data handling adhered to the requirements stated in the European Union’s General Data Protection Regulation.
Intervention
The 3 rounds of sailing, each lasting 10 days, entailed cruising in Scandinavian waters (North Sea, Skagerrak, Kattegat), sailing from Denmark to Scotland, and sailing from Scotland to Denmark. Participants spent an average of 107.5 hours at sea (16 hours on light seas, 28 hours on moderate seas, and 63.5 hours on heavy seas) acting as crew members under the supervision of 3 experienced and licensed sailors. Daily onboard tasks included helming, navigation, on-watch duty, boat maneuvers (eg, trimming, hoisting and lowering sails, handling of anchor and moorings), cooking, and cleaning. All boat-handling tasks were performed manually; no electronic or hydraulic aids were available. Aside from the study participants, additional people were on board, including a medical doctor, members of the research team, and people with MS who were not participating in the study. All crew members performed 9-hour watch cycles of 3 hours of on-deck watch duty, 3 hours as standby/lookout, and 3 hours off duty. Participants who were unable to stay on deck (eg, due to seasickness or fatigue) were allowed to switch shifts with other participants. Adverse events were monitored during the sailing intervention. The severity of seasickness was reported subjectively by the participants. Intervention adherence was evaluated by the number of completed work sessions (on-deck duty or standby/lookout). No minimum adherence threshold was defined; the data for all participants have been included in the analysis.
Experimental Protocol
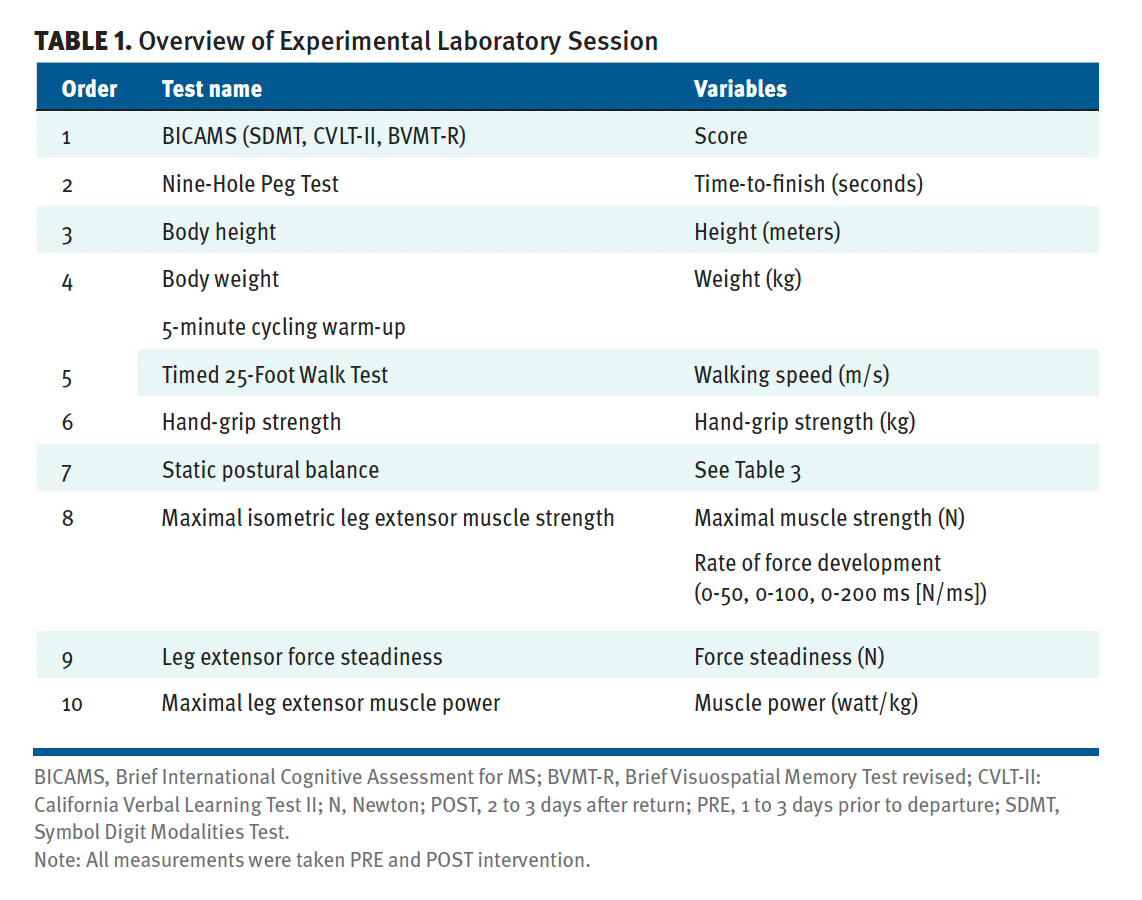
Participants visited the laboratory for a single test session 1 to 3 days prior to sailing (PRE), with another session performed following the intervention period (POST; 1-3 days after return). Each laboratory session lasted approximately 2 hours. Upon arrival at the laboratory, participants were allowed to rest, then were familiarized with the tests by performing submaximal attempts of all tasks. The testing sequence was standardized to minimize the accumulation of fatigue, ie, no/low fatiguing tests performed prior to highly fatiguing tests (Table 1).
Table 1. Overview of Experimental Laboratory Session
Leg Extensor Muscle Strength and Rapid Force Capacity
Maximal isometric unilateral leg extensor contractions (MVC) were performed with the participants seated in a rigid custom-built leg-press device.13 The subjects were seated (with hip joint angle at approximately 90°, knee joint angle at 60° flexion [0° = full extension] measured with a manual goniometer), with 1 foot in a standardized position on a fixed footplate instrumented by force transducers. Participants kept their arms crossed over their chests and were instructed to avoid movements with their arms or upper bodies. They were instructed to push as hard and fast as possible,14 and to maintain their maximal effort for 3 to 5 seconds, while receiving strong verbal encouragement from the test leader. Online visual feedback of the force signal was provided on a computer screen. Three MVC trials were performed for each leg, separated by 45- to 60-second rest periods; however, additional trials were carried out if the peak force was 5% greater than that of the previous trial. Data were sampled digitally (1000-Hz sampling frequency) and filtered using a digital, zero-lag, fourth-order, 15-Hz lowpass Butterworth filter. The trial with the greatest peak force was selected for subsequent data analysis (peak force and rate of force development).
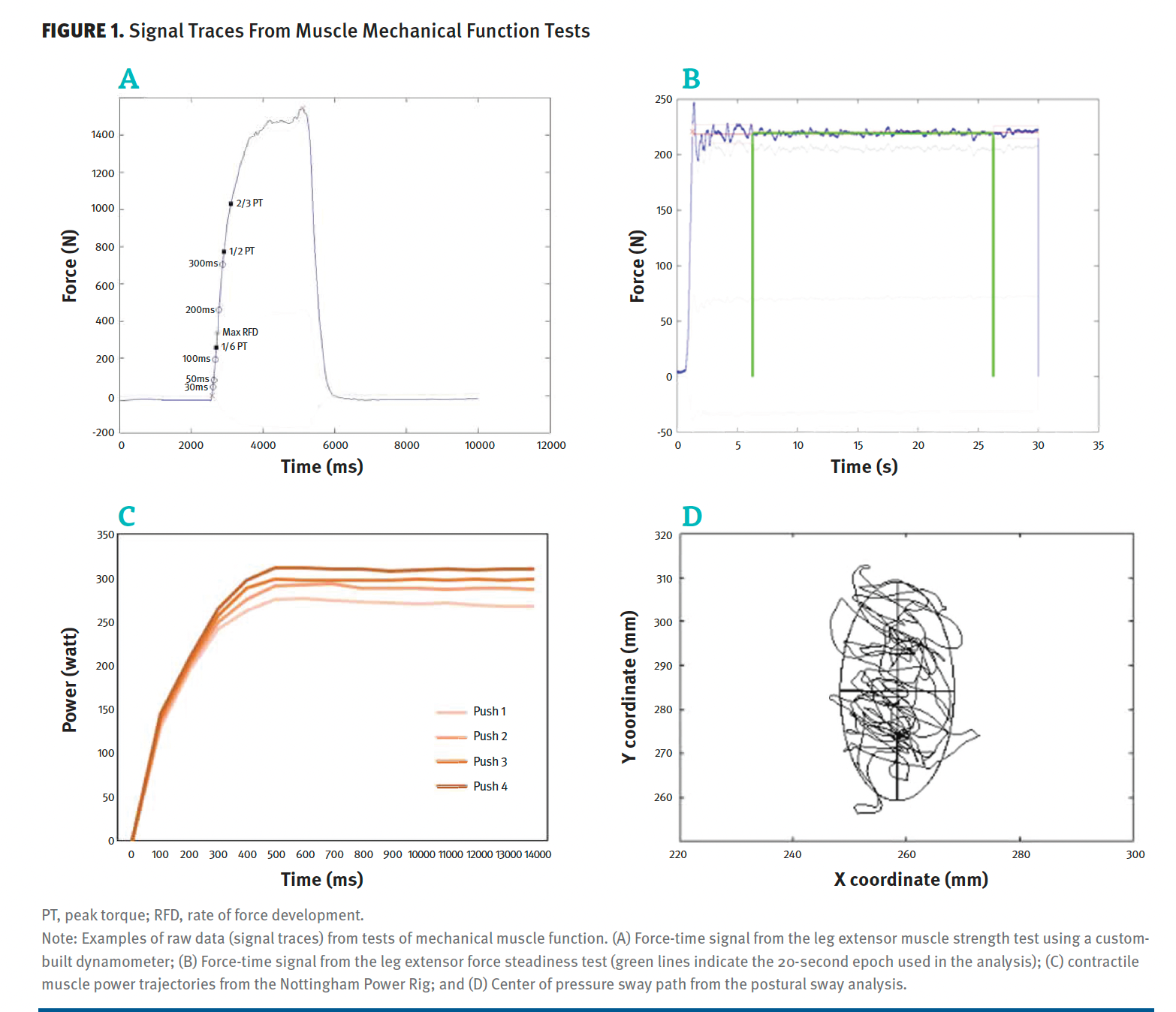
Rapid force capacity, assessed as contractile rate of force development (RFD), was determined as the average slope of the force-time curve in predetermined time intervals of 0 to 50 ms, 0 to 100 ms, and 0 to 200 ms following onset of contraction (0 ms),15,16 which in turn was determined as the time point at which the force exceeded 2% of peak force above the baseline (Figure 1).15
Figure 1. Signal Traces From Muscle Mechanical Function Tests
Force Steadiness
Following MVC testing, 2 unilateral sustained leg extensor contractions (30 sec, 10% of peak force) were carried out for each leg (Figure 1).17 While receiving online feedback on the computer screen, participants were instructed to produce a constant force (10% MVC force) by matching a horizontal line (target force) on the monitor.18 For the post hoc analysis of steadiness, force data (signal treatment, as described above) were extracted from a 20-second period after the onset of steadiness (the time point at which the force output exceeded the median force of the entire signal), with force steadiness subsequently calculated as the SD of the mean force within the 20-second time interval.17 All force signals were visually inspected for irregularities, and the trial for each leg with the lowest 20-second average SD (ie, the highest degree of steadiness) was reported.
Contractile Power
Maximal unilateral leg extensor muscle power (LEP) was assessed with the Nottingham Power Rig (Figure 1), as previously reported.19 In brief, the seat was individually adjusted to achieve an end position of 10° knee-joint flexion. Participants were sitting upright with arms crossed over their chests and with 1 foot resting on the pedal. Participants were instructed to push as hard and as fast as possible14 on the pedal connected to an inertial flywheel while receiving strong verbal encouragement and visual feedback. Trials were discarded if any countermovement was observed. Each trial was separated by 45 to 60 seconds, and additional trials (up to 6) were given until a drop in power occurred (on average, 4.2 ± 0.8 trials were carried out). The trial with the greatest average power (W) normalized to body weight (W/kg) was selected for statistical analysis.
Postural Balance
Postural balance was assessed during 30-second static bilateral standing on a force platform (Kistler 9281 B, Winterthur, Switzerland; Figure 1).20 Participants were instructed to stand still for 30 seconds while focusing on a fixed point (elevated 1.65 meters and 3 meters in front of the participant), with feet at hip width and arms akimbo. Participants performed 2 attempts separated by 1 to 2 minutes of rest. The trial with the shortest total sway length of the center of pressure (COP) was selected for post hoc analysis. The analogue force signals were sampled using an external 16-bit A/D converter. They were later processed to calculate the following sway variables: total COP sway length, COP sway area, and confidence ellipse area.20 Further, postural balance was evaluated by calculating the variability (SD) in anterior-posterior (A-P/SDy) and medio-lateral (M-P/SDx) COP displacement.20
Hand-Grip Strength
Maximal unilateral hand-grip strength was measured for both hands with a hydraulic hand dynamometer (Baseline LiTE, Fabrication Enterprises). Participants were positioned upright against a wall with the elbow at 90° flexion, such that the upper arm and elbow were supported by the wall. The participants squeezed as hard as possible14 without countermovement, while strong verbal encouragement was provided. A minimum of 3 trials were performed with 60 seconds of rest between successive trials, and additional trials were carried out if a significant improvement occurred on the last trial. The trial with the highest measured strength (kg) was noted.
Walking Capacity
The Timed 25-Foot Walk test was used for the assessment of walking function.21 A 25-foot course was set up with participants standing behind the starting line and walking past the finish line to prevent deceleration toward the end. The time was recorded from when the participant first lifted their foot until the first foot crossed the finish line. Two trials were performed, and the average of these trials was reported.21
Manual Dexterity
Participants were also asked to complete the Nine-Hole Peg Test (9-HPT) test.22 In brief, participants were asked to take pegs from the box and, as quickly as possible, place the pegs onto a board until completely full and subsequently relocate pegs to the box as fast as possible. Two trials were conducted with each hand. The time to complete the task was registered, and the fastest time was recorded.
Cognitive Assessments
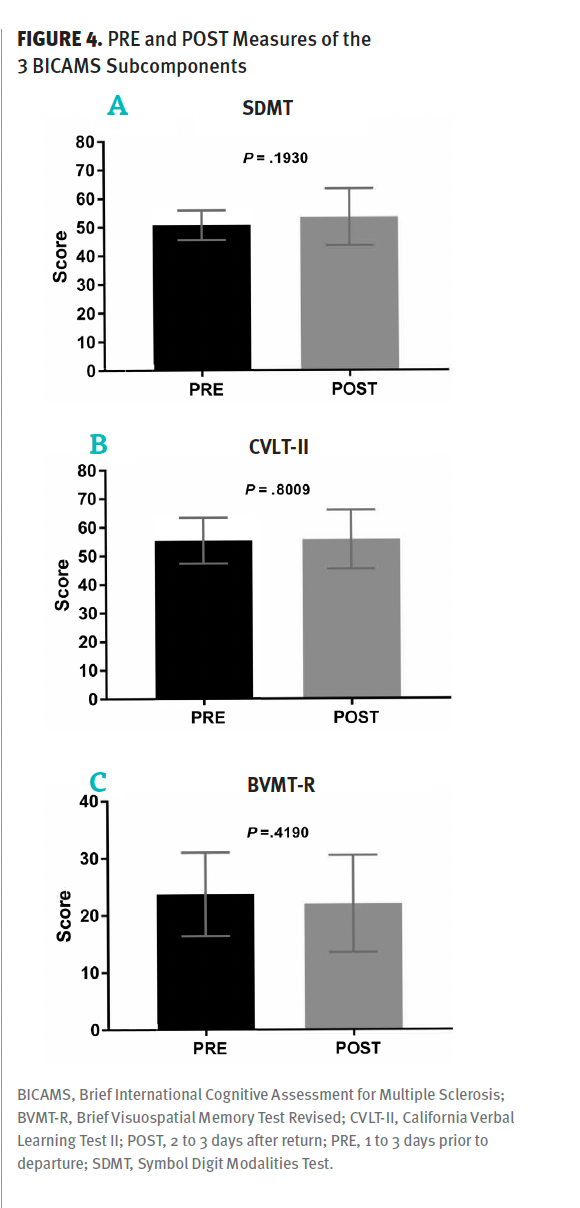
We used the Brief International Cognitive Assessment for MS (BICAMS),23 which consists of 3 cognitive tests that we carried out as recommended: Symbol Digit Modalities Test, California Verbal Learning Test II, and Brief Visuospatial Memory Test revised. Scores for each individual subcomponent of BICAMS were included for further statistical analysis.
Statistical Analysis
PRE to POST changes in various outcome variables were assessed using a paired t test or Wilcoxon signed rank test, depending on the presence of Gaussian or non-Gaussian data distribution, respectively, as assessed visually using quantile-quantile plots and Shapiro-Wilk testing in cases of uncertainty. Data are presented as group means plus or minus SD or median (interquartile range), depending on distribution for both the strongest and weakest extremity. Effect sizes were calculated and interpreted using Cohen d.24
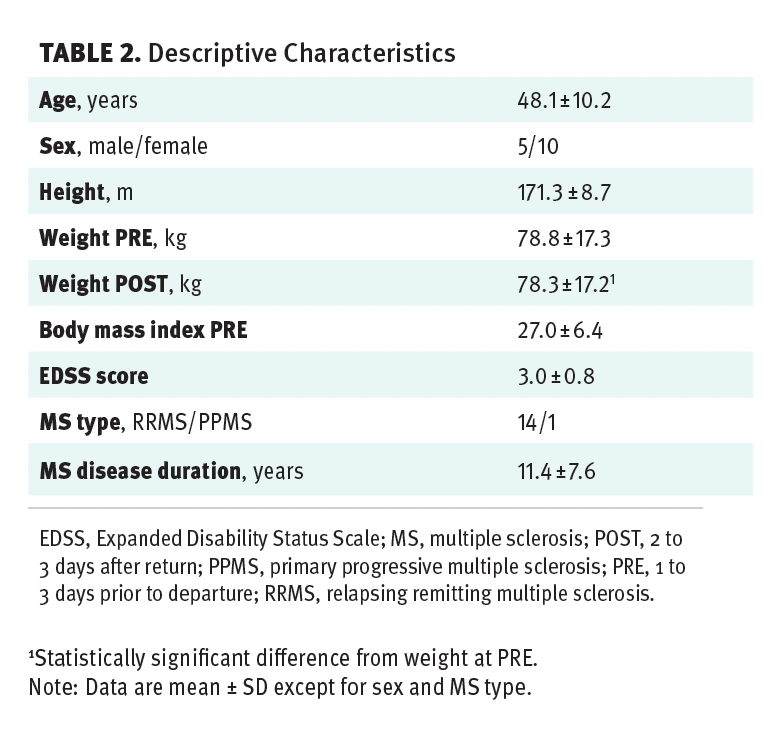
Adverse events included mild or moderate seasickness (n = 10). No serious adverse events or dropouts were reported. Adherence was 100%, as all participants completed all their scheduled work sessions, although 2 individuals had to switch work schedules on 2 occasions due to moderate seasickness. A 0.6% reduction in body weight was observed from PRE (78.8 ± 17.3 kg) to POST (78.3 ± 17.2 kg) (95% CI, 0.01-0.96; P = .046) (Table 2).
Table 2. Descriptive Characteristics
No significant PRE to POST changes in MVC, RFD, LEP, or force steadiness were observed (Figure 2). No significant changes in maximal gait speed or hand-grip strength were found from PRE to POST (cf. Figure 3). As shown in Figure 3, a significant improvement was observed PRE to POST for the strongest hand during the dexterity test (9-HPT) (–1.52 seconds; 95% CI, –2.35 to –0.68; P < .01), while absent for the weakest hand (P = .93). No significant changes were found from PRE to POST for any of the postural sway parameters (Table 3). Likewise, no significant changes were observed for the BICAMS tests (Figure 4). No statistically significant changes were observed in any outcome measurements from the POST test to the 3-month follow-up assessment (data not shown).
Figure 2. PRE and POST Measures of Muscle Mechanical Function
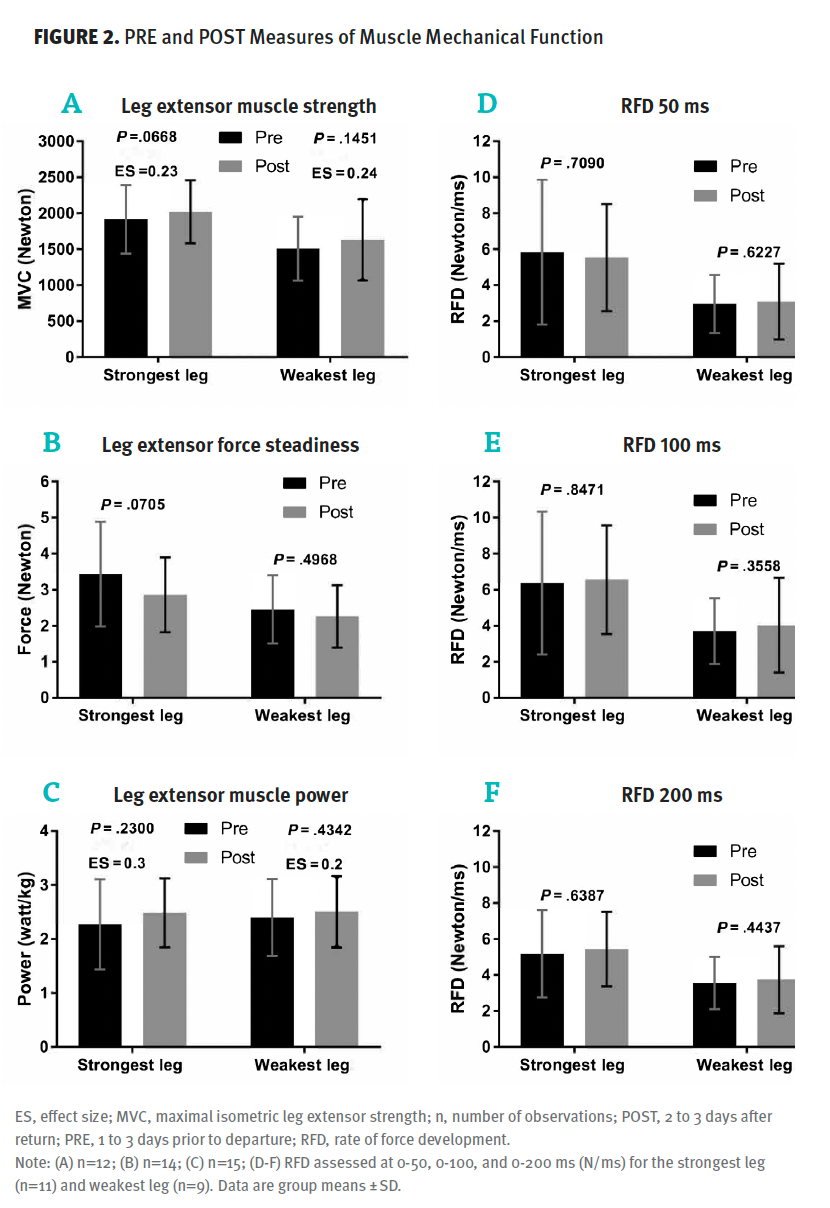
Figure 3. PRE and POST Measures
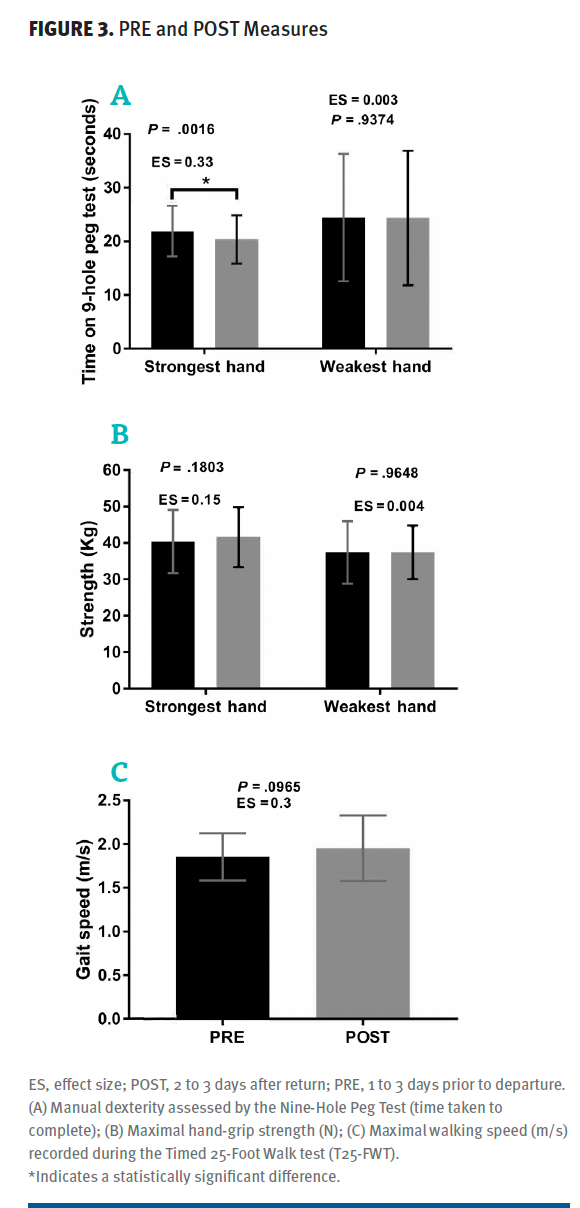
Table 3. Postural Sway
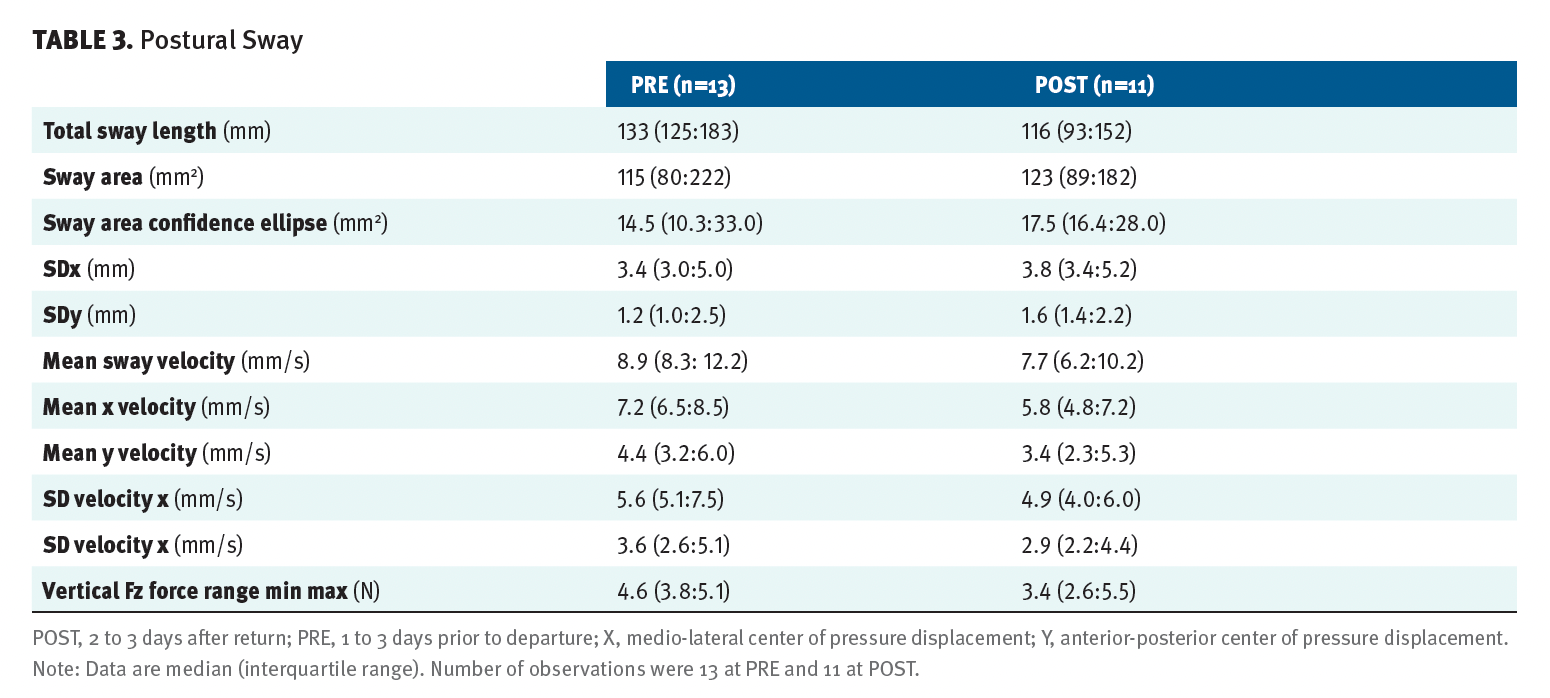
Figure 4. PRE and POST Measures of the 3 BICAMS Subcomponents
The present study explored the effects of a 10-day continuous ocean sailing intervention for improving lower-limb mechanical muscle function, functional capacity, fine motor control, postural balance, and cognitive function in people with MS. Notably, no systematic changes in mechanical muscle function, functional capacity, postural balance, or cognition were observed in response to the intervention protocol. However, no deteriorations in these parameters were observed either, and there were only a few minor adverse events during the sailing intervention (seasickness), with no serious adverse effects and no participants who dropped out. Additionally, adherence (assessed as the number of completed scheduled work sessions) was 100% for all participants. Taken together, this indicates that ocean sailing may be considered to be feasible for mildly to moderately impaired adults with MS (age 48.1 ± 10.2 years, EDSS 3.0 ± 0.8), as it does not seem to produce impairments in functional capacity or lower-limb mechanical muscle function, respectively. Whether more prolonged intervention protocols may evoke positive changes or if more severely impaired people with MS can engage safely in ocean sailing remains unknown.
MS causes impaired sensorimotor function, thus compromising postural balance, which is associated with increased risk of falling.25 The chronically increased inflow of afferent signals to the CNS that likely occurs when navigating on a sailing yacht requires individuals to continuously react to afferent input from the PNS and modulate efferent motor output to maintain sufficient postural stability. Postural sway is influenced by inputs from the vestibular system, the somatosensory system, and the visual sensory system. As ocean sailing challenges all these systems and imposes demands for adequate levels of motor control, it follows that adaptive changes in any of these systems might occur, in turn evoking improvements in postural stability and neuromuscular function. Nonetheless, fine motor control (force steadiness) and postural sway parameters remained unaltered following the sailing intervention, which suggests that no changes occurred in postural motor control or in somatosensory inflow to the CNS in the present study. The 1.52-second average improvement observed for the manual dexterity of the strongest hand did not exceed a level considered clinically relevant.26 Although no other improvements were observed following the intervention, it should be noted that no reductions or deteriorations were observed for any of these outcome variables.
To the best of our knowledge, on-water sailing intervention studies have never been performed in people with neurological disorders. One sailing-simulation–based rehabilitation study in people with spinal cord injury showed improvements in balance and questionnaire-assessed mobility and quality of life after 30 to 40 minutes of virtual sailing 3 times a week for 6 weeks.27 Interestingly, their training program was more similar to classic aerobic conditioning or resistance training programs (in terms of volume, frequency, and intensity), which previously have been successfully applied in this population.6,28 Previous findings in reports regarding people with MS have demonstrated increases in RFD after 24 weeks of resistance training29 and improvements in dynamic balance after 10 weeks of resistance training or balance training.30 In contrast, no changes were observed in RFD or postural balance in the present study. Thus, while ocean sailing mainly consists of low-intensity yet high-volume (chronic) periods of physical activity, a higher intensity of afferent sensory input and efferent motor output may be required in future sailing intervention protocols to induce measurable adaptations in sensory-motor function and maximal muscle strength, power, and RFD in people with MS.
A minor (≈1%), albeit significant, decrease in body weight occurred, which likely reflects the elevated energy expenditure associated with offshore sailing.31 Although this decrease in body weight is too small to be considered clinically relevant, it highlights the elevated nutritional requirements during
ocean sailing.
It is commonly stated that people with MS enter a vicious cycle of decreased functional capacity as a result of their MS symptoms, resulting in an associated decline in physical activity levels. It was hypothesized that a positive experience during sailboat circumnavigation would enhance physical well-being, thereby increasing physical activity and exercise engagement during and following the intervention period. Although previous studies have found improvements in self-efficacy and quality of life after specific sailing intervention protocols in people with psychosocial disabilities,32,33 increases in MS-related fatigue following the intervention could counter such effects by reducing physical activity levels. In the present study, comparisons between the POST intervention and the 3-month follow-up assessment did not reveal any significant changes for any of the outcome parameters; however, measurements of physical activity, physical well-being, and other psychosocial outcomes were not included. Thus, it is unknown how long-term ocean sailing affects physical activity levels and psychosocial outcomes following return to land.
Study Limitations
The present exploratory study was limited by the lack of a non-sailing control group and a small sample size (ie, low statistical power), as well as a lack of physical activity measurements in the period following the intervention protocol. Given the small sample size, the reported effect sizes should be interpreted cautiously. Larger and/or more prolonged studies are needed to examine whether levels of physical activity or fatigue are elevated during more prolonged ocean sailing interventions and to clarify if this may be associated with gains in physical well-being, physical function, and overall health. Further, while mechanical muscle function and physical performance outcomes are important for the ability to perform activities of independent daily living, other outcome measurements may be more sensitive to small changes from given sailing intervention protocols (eg, postural sway during sudden perturbations).
Ten days of ocean sailing did not seem to have any measurable effects on lower-limb mechanical muscle function or any positive effect on functional performance or cognitive capacity in people with MS. Notably, however, mechanical muscle function and functional capacity were not negatively affected by the 10-day sailing protocol. Although 1 notable adverse event was reported by a few participants (seasickness), there were no serious adverse events or dropouts, and participants completed all scheduled work sessions. Thus, ocean sailing seems to represent a safe and tolerable intervention strategy for people with MS who experience mild to moderate impairments.
Acknowledgments: The authors would like to thank Michala Kolind Holm, Mikkel Beltoft Lund, Mie Kastrup Christensen, and Maria Krüger for their assistance with data collection, and Henrik Baare Olsen for his assistance with data processing.
Prior Presentation: Part of the material was presented as a digital poster at the European Committee for Treatment and Research in Multiple Sclerosis meeting; September 18-20, 2024; Copenhagen, Denmark.
Declaration of Conflicting Interest: The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: This study was funded by the Trigon Foundation.
Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. Multiple sclerosis. N Engl J Med. 2000;343(13):938-952. doi:10.1056/NEJM200009283431307
Anthonisen M. Oceans of Hope. Accessed September 11, 2024. https://www.oceansofhope.org/english/
Broadbent FJ, Swalwell JM. “I can do more than I thought I could”: exploring the online blogs from the Sailing Sclerosis Oceans of Hope journey. Disabil Rehabil. 2020;42(6):880-886. doi:10.1080/09638288.2018.1510046
Farup J, Dalgas U, Keytsman C, Eijnde BO, Wens I. High intensity training may reverse the fiber type specific decline in myogenic stem cells in multiple sclerosis patients. Front Physiol. 2016;7:193. doi:10.3389/fphys.2016.00193
Wens I, Dalgas U, Vandenabeele F, et al. High intensity exercise in multiple sclerosis: effects on muscle contractile characteristics and exercise capacity, a randomised controlled trial. PloS One. 2015;10(9):e0133697. doi:10.1371/journal.pone.0133697
Dalgas U, Langeskov-Christensen M, Stenager E, Riemenschneider M, Hvid LG. Exercise as medicine in multiple sclerosis-time for a paradigm shift: preventive, symptomatic, and disease-modifying aspects and perspectives. Curr Neurol Neurosci Rep. 2019;19(11):88. doi:10.1007/s11910-019-1002-3
Taul-Madsen L, Connolly L, Dennett R, Freeman J, Dalgas U, Hvid LG. Is aerobic or resistance training the most effective exercise modality for improving lower extremity physical function and perceived fatigue in people with multiple sclerosis? A systematic review and meta-analysis. Arch Phys Med Rehabil. 2021;102(10):2032-2048. doi:10.1016/j.apmr.2021.03.026
Šilarová A, Hvid LG, Hradílek P, Dalgas U. Exercise-induced heat sensitivity in patients with multiple sclerosis: definition, prevalence, etiology, and management-a scoping review. Mult Scler Relat Disord. 2024;90:105827. doi:10.1016/j.msard.2024.105827
Branth S, Hambraeus L, Westerterp K, et al. Energy turnover in a sailing crew during offshore racing around the world. Med Sci Sports Exerc. 1996;28(10):1272-1276. doi:10.1097/00005768-199610000-00010
Bojsen-Møller J, Larsson B, Aagaard P. Physical requirements in Olympic sailing. Eur J Sport Sci. 2015;15(3):220-227. doi:10.1080/17461391.2014.955130
Manzanares A, Camblor Á, Romero-Arenas S, Segado F, Gil-Arias A. Adapted sailing teaching methodology using vsail-trainer simulator as rehabilitation therapy. A feasibility study. J Spinal Cord Med. 2024;47(6):960-967. doi:10.1080/10790268.2023.2228585
Aprile I, Iacovelli C, Iuvone L, et al. Use of a virtual-technological sailing program to prepare children with disabilities for a real sailing course: effects on balance and quality of life. J Child Neurol. 2016;31(8):1074-1080. doi:10.1177/0883073816638756
Benedict RHB, Amato MP, Boringa J, et al. Brief International Cognitive Assessment for MS (BICAMS): international standards for validation. BMC Neurol. 2012;12:55. doi:10.1186/1471-2377-12-55
Sandroff BM, Sosnoff JJ, Motl RW. Physical fitness, walking performance, and gait in multiple sclerosis. J Neurol Sci. 2013;328(1-2):70-76. doi:10.1016/j.jns.2013.02.021
Caserotti P, Aagaard P, Larsen JB, Puggaard L. Explosive heavy-resistance training in old and very old adults: changes in rapid muscle force, strength and power. Scand J Med Sci Sports. 2008;18(6):773-782. doi:10.1111/j.1600-0838.2007.00732.x
Maffiuletti NA, Aagaard P, Blazevich AJ, Folland J, Tillin N, Duchateau J. Rate of force development: physiological and methodological considerations. Eur J Appl Physiol. 2016;116(6):1091-1116. doi:10.1007/s00421-016-3346-6
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol Bethesda MD 1985. 2002;93(4):1318-1326. doi:10.1152/japplphysiol.00283.2002
Bojsen-Møller J, Magnusson SP, Rasmussen LR, Kjaer M, Aagaard P. Muscle performance during maximal isometric and dynamic contractions is influenced by the stiffness of the tendinous structures. J Appl Physiol (1985). 2005;99(3):986-994. doi:10.1152/japplphysiol.01305.2004
Hortobágyi T, Tunnel D, Moody J, Beam S, DeVita P. Low- or high-intensity strength training partially restores impaired quadriceps force accuracy and steadiness in aged adults. J Gerontol A Biol Sci Med Sci. 2001;56(1):B38-B47. doi:10.1093/gerona/56.1.b38
Tracy BL, Dinenno DV, Jorgensen B, Welsh SJ. Aging, visuomotor correction, and force fluctuations in large muscles. Med Sci Sports Exerc. 2007;39(3):469-479. doi:10.1249/mss.0b013e31802d3ad3
Bassey EJ, Short AH. A new method for measuring power output in a single leg extension: feasibility, reliability and validity. Eur J Appl Physiol. 1990;60(5):385-390. doi:10.1007/BF00713504
Jakobsen MD, Sundstrup E, Krustrup P, Aagaard P. The effect of recreational soccer training and running on postural balance in untrained men. Eur J Appl Physiol. 2011;111(3):521-530. doi:10.1007/s00421-010-1669-2
Feys P, Lamers I, Francis G, et al. The Nine-Hole Peg Test as a manual dexterity performance measure for multiple sclerosis. Mult Scler. 2017;23(5):711-720. doi:10.1177/1352458517690824
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Routledge; 2013. doi:10.4324/9780203771587
Cameron MH, Lord S. Postural control in multiple sclerosis: implications for fall prevention. Curr Neurol Neurosci Rep. 2010;10(5):407-412. doi:10.1007/s11910-010-0128-0
Hervault M, Balto JM, Hubbard EA, Motl RW. Reliability, precision, and clinically important change of the Nine-Hole Peg Test in individuals with multiple sclerosis. Int J Rehabil Res. 2017;40(1):91-93. doi:10.1097/MRR.0000000000000209
Manzanares A, Camblor Á, Romero-Arenas S, Segado F, Gil-Arias A. Effect of a semi-immersive virtual reality navigation therapy on quality of life in persons with spinal cord injury. Disabil Rehabil Assist Technol. 2023;18(6):730-735. doi:10.1080/17483107.2021.1913520
Riemenschneider M, Hvid LG, Ringgaard S, et al. Investigating the potential disease-modifying and neuroprotective efficacy of exercise therapy early in the disease course of multiple sclerosis: the Early Multiple Sclerosis Exercise Study (EMSES). Mult Scler. 2022;28(10):1620-1629. doi:10.1177/13524585221079200
Kjølhede T, Vissing K, de Place L, et al. Neuromuscular adaptations to long-term progressive resistance training translates to improved functional capacity for people with multiple sclerosis and is maintained at follow-up. Mult Scler. 2015;21(5):599-611. doi:10.1177/1352458514549402
Callesen J, Cattaneo D, Brincks J, Kjeldgaard Jørgensen ML, Dalgas U. How do resistance training and balance and motor control training affect gait performance and fatigue impact in people with multiple sclerosis? A randomized controlled multi-center study. Mult Scler. 2020;26(11):1420-1432. doi:10.1177/1352458519865740
Allen JB, Jong MRD. Sailing and sports medicine: a literature review. Br J Sports Med. 2006;40(7):587-593. doi:10.1136/bjsm.2002.001669
Sancassiani F, Cocco A, Cossu G, et al. “VelaMente?!” - sailin in a crew to improve self-efficacy in people with psychosocial disabilities: a randomized controlled trial. Clin Pract Epidemiol Ment Health. 2017;13:200-212. doi:10.2174/1745017901713010200
Carta MG, Maggiani F, Pilutzu L, et al. Sailing for rehabilitation of patients with severe mental disorders: results of a cross over randomized controlled trial. Clin Pract Epidemiol Ment Health. 2014;10:73-79. doi:10.2174/1745017901410010073



























