Practice Points
- This feasibility study provides preliminary evidence on the applicability of an occupation-based intervention for upper extremity function for people with multiple sclerosis.
- Collaborative goal setting in occupation-based interventions may increase patients’ motivation to participate in the rehabilitation program.
People with multiple sclerosis (MS) may confront complex motor, sensory, visual, cognitive, and psychological symptoms.1 In recent decades, numerous studies have focused on lower extremity functioning, gait, and balance changes that occur in the early stages of MS. However, there have been few studies that examine hand and upper extremity function changes in people with MS.2 Approximately three-quarters of people with MS have demonstrated upper extremity dysfunction on 1 or both sides of their bodies.3,4 Upper extremity dysfunction contributes to reducing the ability to perform activities of daily living and is an important predicator of overall activity and participation within the community,5 possibly resulting in decreased independence and lower quality of life.6
Several rehabilitation interventions have been developed to address upper extremity dysfunction, such as exercise training, task-oriented training, sensory training, robotics, and constraint-induced movement therapy. According to a systematic review, however, there is a lack of sufficient evidence of improvement, perhaps because the interventions do not target the upper extremity exclusively.2
Occupational therapists are rehabilitation team members who focus on improving occupational performance through occupation-based interventions (OBIs). OBI is a patient-centered practice in which the occupational therapist, in collaboration with the patient, chooses interventions based on the patient’s interests, needs, health, and participation in daily life.7
OBI provides a holistic and a strong base for patients to achieve their occupational therapy goals, enhances the ability of therapists to communicate with their patients, and can improve patients’ satisfaction with services.8 However, occupation-based therapies are somewhat culture dependent, so it is necessary to investigate their effectiveness in different cultures.9 Some barriers to using OBI are that therapists lack the knowledge and skills to implement the theory into practice,8 preference for the dominant medical model, patient request, lack of resources, environmental context,10 culture,11 and time required for goal setting.12
Preliminary evidence supports the effectiveness of OBI for people with some degenerative and neurologic diseases such as stroke or a traumatic brain injury.13 The aim of this study is to describe the development and content of an OBI program focused on hand function that was used to improve the occupational performance of 2 Iranian women with MS.
Methods
This feasibility study evaluated the effect of OBI for hand function on 2 women with MS from the Isfahan MS Society. Both volunteers were examined by a neurologist to determine the type of MS they have and their level of disability.
After explanations of the purpose of the study, written consent was obtained from both of the participants and they were assured that their information would be kept confidential. This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences under the code of ethics IR.USWR.REC.1396.319.
Participants
Participant 1 was a divorced woman, aged 41 years, with an undergraduate education. Her MS was diagnosed 9 years ago. She has no income or insurance and lives with her mother. According to her report, the strength and coordination of movement in her hands and upper extremities has worsened with the progression of MS symptoms. She needs help in home maintenance and self-care, including bathing and hair brushing.
Participant 2 was a woman, aged 50 years. Her MS was diagnosed 12 years ago. She states that she feels numbness and tingling, and has decreased hand strength and endurance. Sometimes she is responsible for taking care of her grandson and her mother-in-law, who had a stroke. She is independent in all her self-care and mobility activities, but struggles with home maintenance activities.
Study Instruments
The Montreal Cognitive Assessment (MoCA) was used because it is more sensitive than the Mini–Mental State Examination in identifying mild cognitive impairment in the general population.14 The Cronbach α of the MoCA has been reported as 0.77; a cutoff score of 24 is considered mild cognitive impairment.15
The Expanded Disability Status Scale (EDSS) was used to evaluate the severity of the participants’ MS. A higher score on this scale indicates a higher degree of severity.16 The validity and reliability of this tool are adequate.17
The Canadian Occupational Performance Measure (COPM) was used to investigate occupational performance.18 It is a valid and reliable tool with acceptable test-retest reliability and content validity that identifies occupational performance problems across the areas of self-care, productivity, and leisure through a semistructured interview.18–20 A self-rated score of 1 indicates minimum performance and satisfaction with performance, and a score of 10 is the highest score.
The 9-Hole Peg Test (9HPT) is the gold standard tool for evaluating hand dexterity. Interrater and test-retest reliability of this test is high.21 Bertoni et al reported a cutoff point of greater than 1.95 SD of the norm.22
The Fatigue Severity Scale (FSS) is a 9-point scale assessing fatigue in people with MS. Lower scores on this scale indicate less fatigue and less impact on everyday life activities. The test-retest reliability of this tool in Iran is 0.93.23 The lowest score possible is 9 and the highest is 63.
Inclusion criteria were a neurologist-determined EDSS score between 3.5 and 5.5 (ie, able to walk independently) and a MoCA score of greater than 24.
Procedure
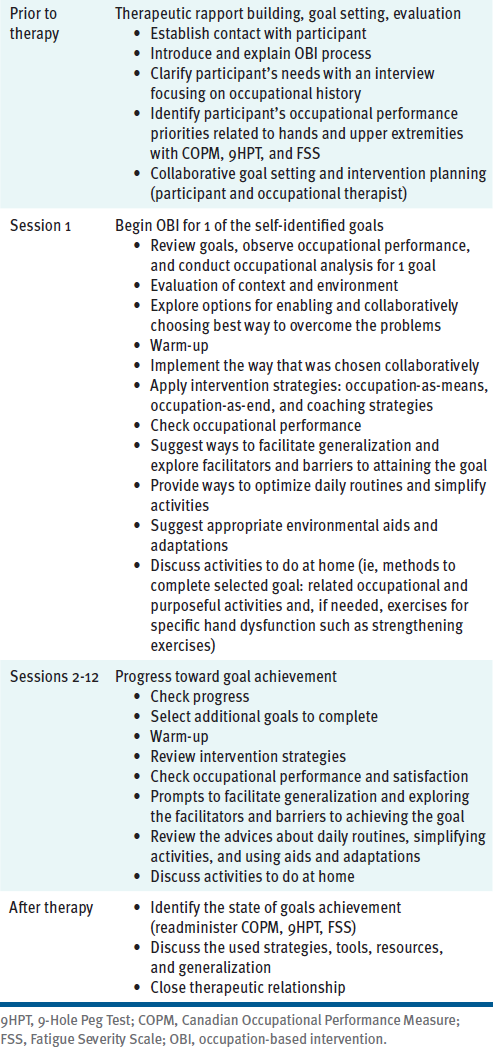
Initially, the primary clinical program was developed based on a comprehensive review of OBIs, as well as the biomechanical model and interventions used in rehabilitation of hand and upper extremities with persons with MS.24 The OBI used in this study guides patients through their self-identified goals regarding their occupational hand function. The developed intervention uses the Model of Human Occupation25 (MOHO) to describe occupational performance and participant involvement; motivation for, as well as patterns and performance of, daily tasks; and the fit between occupational goals, participant ability, and capacity in hand function and environment.26 The therapist used MOHO strategies to support the participants, including validating, identifying, giving feedback, advising, negotiating, structuring, coaching, encouraging, and providing physical support.26 In addition, solution-focused coaching,27 adult learning theory,28 solution-focused therapy,29 and self-management30 were used as components of the intervention. Each session was approximately 1 hour and occurred 2 times a week for 6 weeks. The content of the sessions was based on the participants’ selected goals and priorities based on the COPM (Table 1).
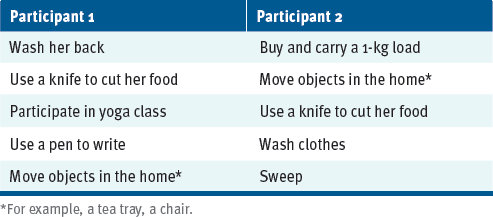
At the first session, both participants chose their own goals (Table 2). In the second session, the therapist asked them about how they did activities in the past, observed how these tasks were currently performed, and discussed how performance could be improved by asking reflective questions. During the sessions, the emphasis was on self-assessment. The occupational therapist and patient also discussed ways to promote the construction of a daily routine, to return to a healthy routine, to develop positive habits to save energy, to increase ways to be active for a longer time, and methods to prevent fatigue. When the goals were achieved, the next goal was examined. Reevaluation was conducted in the week after attaining the goal.
Validity of the OBI Program
The validity of the OBI program was investigated in interviews with 5 occupational therapists who had at least 5 years of clinical experience focused on OBI. The experts evaluated the validity of the intervention program rating the simplicity, clarity, relevance, and necessity of the program on a Likert scale. They were asked to recommend suggestions, corrections, or additions. The experts had an average work experience of 10.2 (SD = 3.4) years. Three of them had a doctorate degree, 1 had a master’s degree, and 1 had a bachelor’s degree; 4 were women. Analysis of the experts’ opinions showed that the program was written simply and clearly and that all written content was essential and relevant.
Results
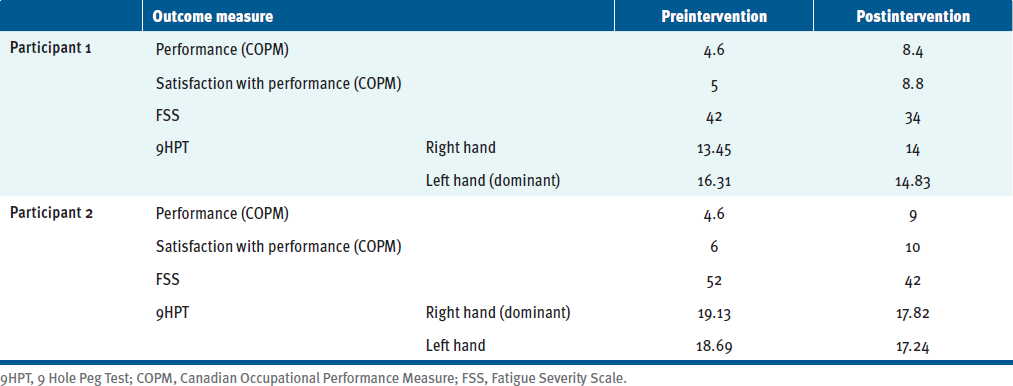
Table 3 descriptively summarizes the COPM, 9HPT, and FSS data. MoCA scores indicated mild cognitive impairment for participant 2 and no cognitive impairment for participant 1. Both participants had an EDSS score of 3.5, indicating moderate disability but no walking impairment. Participant 1 and participant 2 achieved their goals in 8 and 10 sessions, respectively, confirmed by the changes in COPM scores. Both participants had an increase of more than 2 points for both performance and satisfaction, indicating that the OBI intervention made a difference in goal obtainment.
Discussion
The results of this study indicate an improvement in goal performance and performance satisfaction for both participants, as a change of more than 2 points on the COPM31 is clinically meaningful. Likewise, the women’s 9HPT scores reflected improvement in dexterity. FSS scores also indicated reduced fatigue severity for both participants.
In Eastern culture, which includes Iran, people are usually supported by their families during illness, and people with disabilities often come to rely on others for help completing certain tasks and activities of daily living.11 This is juxtaposed with the fact that, in Iran, housework is often performed by women, and women are mostly responsible for caring for other family members. In the context of this study, one of the participants was divorced and the other was responsible for caring for others, so their motivation to achieve maximum hand function was very high.
It was determined that the participants could achieve the goals in 12 sessions of evidence-based, occupation-focused, and patient-centered therapy interventions, but both participants achieved their goals in fewer sessions. The intervention emphasized improving hand and upper extremity performance to meet occupational goals. Using OBI, the occupational therapist collaborated with the participants to help them find new ways to perform daily tasks. The collaboration between the therapist and the participant as well as participant feedback at all stages of the intervention was paramount. The intervention plan was continually adjusted and tailored to the needs of the individual. To ease the process of time-consuming goal setting, a semistructured COPM interview and occupational profile were used.
This was a preliminary study. Generalization would require more robust design. For example, participants in this study did not have significant cognitive problems, so future research should include people with different levels of MS severity in all areas.
Conclusions
This study introduces a simple, structured occupational therapy intervention for people with MS. The improvements in occupational performance, occupational satisfaction, and hand dexterity experienced by both participants suggest that OBI has the feasibility to be implemented with individuals with MS in Iran. More research with a larger sample size is needed to establish the effectiveness of this occupational therapy intervention among a wider population with varying degrees of MS severity and impairment.