Practice Points
- Polypharmacy is prevalent in people with multiple sclerosis and may be associated with adverse cognitive outcomes.
- Disease-modifying therapies, symptomatic treatments, and medications for comorbid conditions contribute to polypharmacy in multiple sclerosis.
- Anticholinergic burden scales like the Drug Burden Index are quick and accessible tools to assess whether medications have unfavorable effects on cognition.
Individuals with multiple sclerosis (MS) experience a wide array of symptoms caused by focal lesions and diffuse neurodegeneration in the central nervous system. It is common for patients to use a disease-modifying therapy (DMT) to slow disease progression as well as treatments for a variety of physical, cognitive, and emotional symptoms.1 For this reason, polypharmacy is a considerable concern for individuals with MS.
Polypharmacy refers to the concurrent use of multiple medications2; it is most commonly quantified in the literature as 5 or more daily medications. Evidence suggests that polypharmacy is associated with adverse health outcomes in those of advanced age, including increased falls, cognitive impairment, and hospitalizations due to drug adverse events.3 Certain types of medications, including those with anticholinergic properties, are particularly hazardous.4 Compared to older adults, individuals with MS represent a similar yet unique population that is vulnerable to polypharmacy effects, yet the literature on this topic is sparse. Our previous research suggests that polypharmacy is associated with subjective cognitive difficulties in MS; however, a consistent relationship with objective cognitive measures was not observed.5
Cognitive abnormalities often emerge as a direct consequence of MS disease pathology, affecting between 40% to 70% of patients.6 Notably, difficulties with cognition can arise at any stage of the disease and tend to persist or worsen over time.7 Common cognitive domains affected in MS include information progressing speed, executive function, and working memory, and these deficits can consequently impair visuospatial abilities and verbal fluency.8 Cognitive symptoms are linked to a range of adverse outcomes in MS, such as problems with activities of daily living, employment, and completing daily household tasks.6
The present study examines the relationship between polypharmacy and objective cognitive performance in adults with MS while accounting for demographic and disease-related factors. We hypothesized that polypharmacy would be negatively associated with cognitive performance, such that people taking more medications would demonstrate poorer performance on objective measures of cognition. We also explored whether anticholinergic burden scales could predict cognitive performance after controlling for relevant covariates.
Methods
Participants
We recruited 90 participants with MS through a large MS specialty clinic affiliated with the University of Kansas Medical Center. Additional recruitment methods included referrals and flyers posted in the clinic. Participants received a $25 Amazon gift card as compensation for their participation. Criteria for inclusion included (1) a confirmed MS diagnosis based on established criteria1 from a board-certified neurologist; (2) no nervous system disorder other than MS; (3) no severe sensory, motor, physical, or neurological impairment that would make participation in the study insurmountable; (4) no history of learning disability; (5) no MS relapse and/or corticosteroid treatment within 4 weeks of evaluation; and (6) access to stable internet in a private location for Zoom teleconferences.
Procedure
Study personnel approached patients with MS while they were attending their routine clinical visits. Upon introduction and a brief description of the research, study personnel assessed patients’ interest in study participation and asked additional screening questions. Eligible and interested patients provided written informed consent, gave their contact information, and scheduled a time to complete the study assessment and questionnaires with the researcher. Out of an abundance of caution during the COVID-19 pandemic, all data collection occurred via telehealth. A battery that could be administered virtually was compiled and included measures across several domains of cognitive functioning that are commonly affected in patients with MS, such as information processing speed, executive functioning, and working memory. The validity and reliability of online assessments using our selected measures has been established in adults with and without cognitive impairment,9 including in MS.10 Participants completed the cognitive assessment portion via Zoom or by telephone if online audio/video connectivity was poor. To ensure that mode of test administration did not unduly influence participant test performance, method of participation was examined as a covariate in analyses. Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at the University of Missouri–Kansas City.11 All procedures were approved by the institutional review boards of the University of Missouri–Kansas City and the University of Kansas Medical Center.
Measures
Medication List
Participants provided a complete list of all medications used daily (including both prescription and over-the-counter drugs), which were tallied to yield the total number of medications (med count). Medications prescribed as prn were only included in analyses if the participant reported taking the medication within 24 hours prior to the testing session. For each medication, participants provided the dosage, frequency, route of administration, date/time of last dose taken, and percentage of doses missed.
The Anticholinergic Burden Calculator (www.anticholinergicscales.es) was used to derive numerical values and qualitative labels (eg, low/medium/high risk) for 3 rating scales thought to be associated with cognitive functioning12: the Anticholinergic Drug Scale (ADS),13 the Anticholinergic Cognitive Burden (ACB) Scale,14 and the Drug Burden Index (DBI).15 For each scale, higher scores indicate increased possibility of anticholinergic impact.
Cognitive Functioning
Verbal memory was assessed using the Hopkins Verbal Learning Test-Revised (HVLT-R).16 We assessed sequential set-shifting with the oral Trail Making Test (OTMT), trials A (processing speed; OTMT-A) and B (executive functioning; OTMT-B).17 The Digit Span test is a subtest of the Wechsler Adult Intelligence Scale–Fourth Edition (WAIS-IV).18 Measures of verbal fluency included both semantic and phonemic fluency tasks.19,20 All measures utilized have been validated for use in individuals with MS.21-26
Physical Functioning
Participants completed the Patient-Determined Disease Steps (PDDS),27 a self-reported measure of disability based on motor and ambulatory dysfunction. The PDDS has 9 levels that range from 0 (normal) to 8 (bedridden). PDDS scores correlate strongly with the Expanded Disability Status Scale (EDSS) and are a valid patient-reported outcome of disability in individuals with MS.28
Comorbidities
We assessed the presence of comorbid health conditions via the Comorbidity Questionnaire for MS, which is validated for use in individuals with MS.29 A supplementary list of comorbidities was also produced to account for other common conditions experienced in the MS population, such as sleep disorder and genitourinary disease; the additional comorbidities were drawn from Cumulative Illness Rating Scale30; Comorbid Medical Conditions Questionnaire31; Charlson Comorbidity Index32; Self-Administered Comorbidity Questionnaire33; and the discussion section of “Validation of a Self-Report Comorbidity Questionnaire for MS.”29 For each patient-reported comorbid condition, follow-up questions included, “What year were you diagnosed?” and “Is this condition currently being treated?” The total number of comorbid conditions per person was tallied to yield a comorbidity score.
Additional Measures
Participants reported the month and year of their MS diagnosis as well as their MS subtype (subtype confirmed by SGL). Demographic information included age, sex, education, ethnicity, and employment status.
Analytic Methods
A composite variable was created for all cognitive measures (ie, HVLT-R Learning, digit span forward [DSF], digit span backward [DSB], OTMT-A, OTMT-B, Phonemic Fluency, and Semantic Fluency) to reduce the number of analyses and thereby decrease the likelihood of family-wise error. This was achieved by transforming the raw scores to standardized z scores, summing the z scores for each measure, and dividing by 7 (ie, the total number of tests). We used negative z scores for OTMT-A and OTMT-B, as higher scores indicate slower performance. This statistical approach has been used frequently in the literature.34-36 We obtained zero-order correlations using Spearman rank correlation (rs); bootstrapping was performed for 1000 samples, yielding 95% CIs for each correlation. Stepwise regression analyses estimated the predictive utility of the polypharmacy indices on the objective cognitive measures. For each model, multiple checks for potential violations of the assumptions for regression analysis were performed. We assessed the normality of residuals by examining predicted probability plots. The assumption of independent errors was checked by examining the Durbin-Watson test statistic. Homoscedasticity was assessed by visual inspection of scatterplots of the predicted values and residuals. We assessed multicollinearity by examining variance inflation factor values.
Analyses were conducted using IBM SPSS Statistics for Windows, Version 27.0. The threshold for statistical significance was set at P < .05.
Results
Preliminary Analyses
Figure S1 (all supplemental material is available in a PDF at the end of the online article) illustrates the enrollment of participants in the study. Demographic and clinical data are presented in Tables S1 and S2, respectively. The study sample included 90 adults with MS. Participants were mostly female (78.9%), White (87.8%), and diagnosed with RRMS (73.3%). Average participant age was 50.71 ± 11.68 years. The median level of disability as measured by PDDS was 2 (IQR = 1, 4). On average, participants took 4.78 ± 3.67 daily medications (range 0-14), and 44.4% (n = 40) met the criteria for polypharmacy. The most common drug categories reported in the sample were DMTs (n = 50, 55.6%), analgesics (n = 42, 46.7%), and antidepressants (n = 40, 44.4%). The most common specific medications in the sample were baclofen (n = 26, 28.9%), gabapentin (n = 17, 18.9%), and levothyroxine (n = 14, 15.6%).
On average, participants reported 3.39 ± 2.87 comorbidities (range 0-13). The most frequent comorbidities were hypertension (n = 28, 31.1%), depression (n = 28, 31.1%), hyperlipidemia (n = 27, 30%), anxiety (n = 17, 18.9%), and migraine (n = 16, 17.8%).
Correlational Analyses
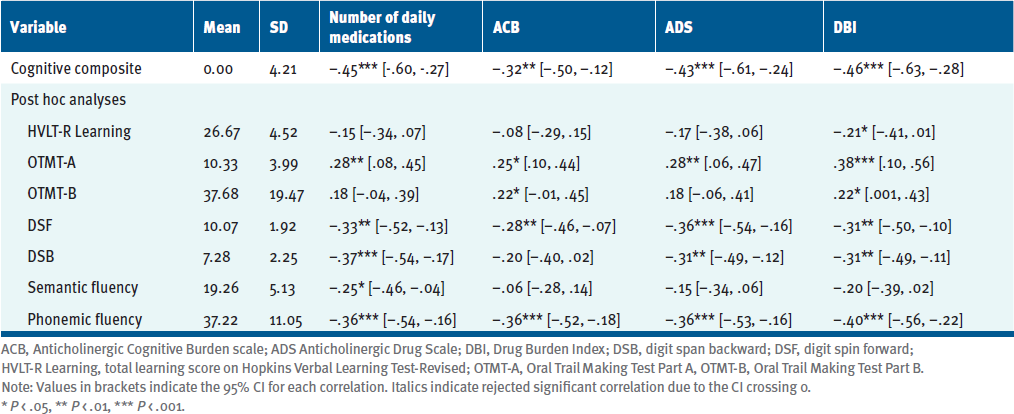
All polypharmacy indices were significantly correlated with each other, with moderately strong (rs = .58, P < .001) to very strong (rs = .85, P < .001) effect sizes (see Table S3). Table 1 displays the correlations between the polypharmacy indices and cognitive performance. Six participants completed the cognitive testing by telephone due to connectivity problems. There were no significant differences in performance based on mode of administration. A greater degree of polypharmacy and anticholinergic burden was associated with worse cognitive performance, with values ranging from rs = –.32, P < .01 (ACB) to rs = –.46, P < .001 (DBI). Post hoc correlations (Table 1) between the polypharmacy scales and each cognitive test were performed to assess whether specific domains of cognition were driving the significant relationships. The polypharmacy indices were more consistently associated with measures of processing speed, attention, and phonemic fluency.
Regression Analyses
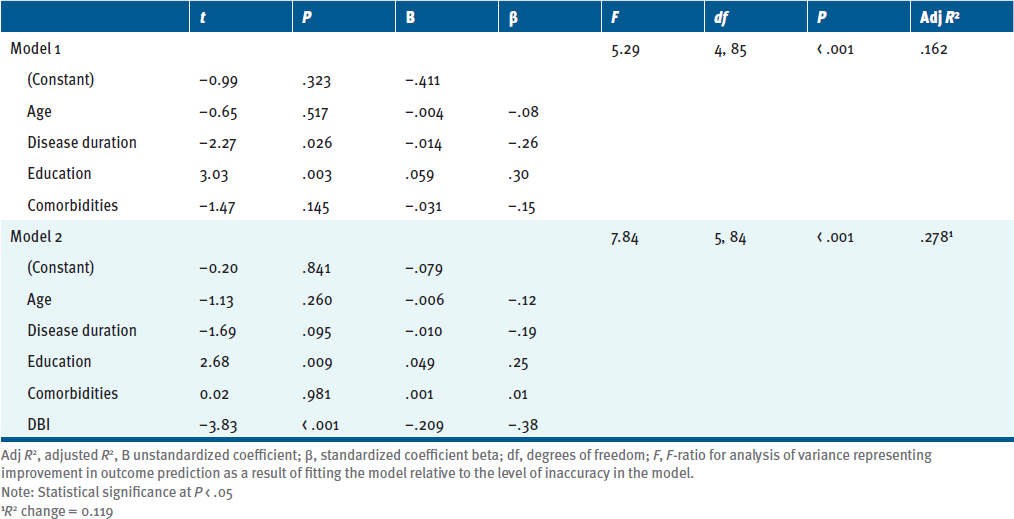
A linear regression was used to examine whether polypharmacy indices predicted composite cognitive performance while controlling for other variables known to be associated with both polypharmacy and cognition. Age, education, disease duration, and comorbidities were entered as covariates in the first block. Polypharmacy indices were entered in the second block using a stepwise method (Table 2). The initial model containing the covariates was significant and explained nearly 20% of the variance in cognitive composite scores, R 2 = 0.199. Disease duration (t = –2.27, P = .026) and education (t = 3.03, P = .003) were both significant predictors in the model. In the second model, DBI was retained and associated with an additional 12% of explained variance (R 2 = .318, ΔR 2 = .119). These results suggest that an individual’s score on the DBI can predict a significant portion of variance in the cognitive composite score, such that for every unit of increase on the DBI index, the cognitive composite z score decreases by .209.
Discussion
Few studies have directly examined polypharmacy in the MS population, and none have examined the potential utility of anticholinergic burden scales in predicting objective cognitive performance. Approximately 44% of the present sample met the criteria for polypharmacy, and DMTs were the most frequently used medications. However, the most commonly reported medication was baclofen, a skeletal muscle relaxant that is commonly used to treat spasticity in MS (and, notably, has considerable anticholinergic properties).
The relationship between anticholinergic medications and cognitive adverse effects in advanced age is well documented across a variety of clinical conditions.14 However, this phenomenon warrants further attention in the MS population. Anticholinergic medications are the first-line treatment for common MS symptoms, such as bladder dysfunction. In a comparison of patients with MS who were and were not using anticholinergic medication for bladder symptoms, Cruce and colleagues reported that anticholinergic users performed significantly worse on measures of processing speed and verbal learning when compared with nonusers.37 This effect remained robust after controlling for age, gender, and disability. More recently, Morrow et al38 used a prospective matched-cohort study to examine the effect of anticholinergic medication on objective cognitive performance in an MS sample. Cases and controls completed a comprehensive neurocognitive battery prior to starting anticholinergic medications and again after 12 weeks. While controls improved on the cognitive measures (consistent with practice effects), the performance of individuals taking anticholinergic medication remained unchanged.
This is the first study to utilize anticholinergic burden scales in the MS population. We compared the number of daily medications to scales that estimate the amount of anticholinergic burden in each participant’s medication regimen. While the ACB and ADS apply numeric ratings to broad lists of medications based on relative anticholinergic activity, the DBI accounts for both sedative and anticholinergic effects and adjusts for medication dosages. We anticipated that scores on these scales (as well as the number of medications) would be highly correlated. This was confirmed, with Spearman correlation coefficients yielding large effect sizes. Of the 3 anticholinergic scales utilized in this study, the DBI yielded the strongest relationship with total number of medications (rs = .75).
Each anticholinergic scale was significantly correlated with the cognitive composite score with moderate to large effect sizes. When examining the relationships between the polypharmacy indices and individual cognitive measures, all scales were correlated with measures of processing speed, attention, and phonemic fluency. This is consistent with the patterns of impaired cognitive performance reported in the studies by Cruce et al37 and Morrow et al,38 as described above.
We then entered all 4 polypharmacy indices in a linear regression to predict cognition, while accounting for the effects of age, disease duration, education, and number of health comorbidities, as these factors are known to be associated with cognitive performance. Our results suggest that the DBI may be useful in predicting objective cognitive performance in adults with MS, as it accounted for roughly 12% of additional variance in cognition above and beyond known covariates. No other polypharmacy index was retained in the regression analysis. Compared to the other polypharmacy indices, the DBI may be best suited to predict cognitive problems due to the inclusion of sedative effects and medication dosage in its calculation of anticholinergic burden.
The relationship between DBI and cognitive performance is inconsistent in the literature. One report found that higher DBI scores were associated with poorer performance on a brief cognitive screening tool in a sample of community-dwelling men ages 70 and older.39 However, another study with a very similar sample found no significant relationship between the DBI and measures of cognitive performance.40 In a sample of diabetic adults, researchers found that DBI scores were associated with poorer memory performance, but only among older adults (> 55 years) in the sample.41 It is possible that such heterogeneous results are attributable to variance in study samples and methods of cognitive assessment.
The current findings are somewhat contrary to our previous work, which found very few differences in objective cognition based on polypharmacy status.5 This discrepancy may be a function of the different cognitive measures utilized in the studies. In our 2014 study, participants completed a battery of assessments during a traditional paper-and-pencil testing session.5 Of these measures, polypharmacy was associated with poorer performance on a measure of prospective memory; however, no other cognitive measures were significantly related to polypharmacy. Due to safety concerns during the COVID-19 pandemic, the present study utilized a different set of cognitive tasks that were appropriate for virtual administration.
Besides utilizing different measures than our 2014 study, the present investigation also computed a composite score based on standardized z scores of the individual cognitive measures, rather than examining each test separately. We also accounted for comorbidities using a more standardized method than in our previous investigations. The most frequently reported comorbidity was hypertension, consistent with our previous research.5
Another notable difference between the present study and our prior work is the composition of the study samples. Our 2014 study was a secondary data analysis of an investigation examining DMT adherence that followed participants for 8 weeks after an initial in-person assessment visit. In contrast, the present study consisted of just 1 virtual study visit and did not require the use of a DMT. It is possible that individuals who agreed to participate in the more intensive study vary systematically from those who participated in the current study, which was less demanding of participants’ time and energy.
Limitations and Future Directions
We recognize several limitations in this study. Generalizability of our results may be limited, given our study sample and the exclusion criteria used in participant recruitment. We excluded individuals with severe motor, sensory, cognitive, or physical impairments that would make study participation insurmountable. Participants were required to have no nervous system disorder other than MS, no history of learning disability, and access to a computer or tablet with a stable internet connection. It is possible that individuals who agreed to participate in the study differ in certain characteristics compared to individuals who declined to participate, such as free time/availability, aversion to cognitive testing, or capacity to engage with technology. The use of virtual data collection due to COVID-19 precautions limits the generalizability of our results to certain demographic groups. For instance, individuals with lower degrees of technological literacy (whether due to older age, poorer cognitive functioning, or socioeconomic status) may be less likely to access and accurately navigate online applications.
Due to the study’s inclusion and exclusion criteria, our sample included relatively few people with more severe disability. This is noteworthy, as individuals with a progressive disease course tend to demonstrate greater cognitive impairment than those with RRMS42 and are more susceptible to polypharmacy and comorbidities.43 Similarly, our sample included relatively few adults over 70 years of age. It is well established in the literature that increased age is associated with polypharmacy and comorbidities, and age-related physiological changes make older adults especially vulnerable to adverse effects related to polypharmacy and anticholinergic medication use.44
Another limitation is related to the virtual data collection method, which precluded the use of certain cognitive tests that are relevant in MS. For instance, measures with visual components are ubiquitous in the traditional assessment of cognition in MS. However, we could not utilize such tests in this study, as we had no way to standardize screen sizes on participants’ computers/tablets or similarly control the testing environment to the degree that is standard in face-to-face assessment. This limitation prevented our ability to measure aspects of visuospatial functioning or utilize certain tests that are known to be sensitive to cognitive impairment in MS. Future studies would benefit from a more comprehensive test battery that includes visually mediated measures, ideally administered in person.
We acknowledge that, due to this study’s correlational and regression-based design, causality cannot be directly addressed. However, ethical implications would preclude methodologies involving randomization of participants to polypharmacy conditions. Alternatively, future longitudinal studies that randomly assign participants to medication review or adjustment may be useful in determining the causal nature of these findings and further inform clinical care. If such studies demonstrate improved cognitive outcomes following medication reduction or reduced anticholinergic load, it may be beneficial to establish clinical guidelines that balance the pros and cons of multidrug therapies and anticholinergic medication use to treat the symptoms of MS. Other potential benefits of reduced medication burden may include reduced medication costs and improved treatment adherence, as demonstrated in other clinical populations.45
Conclusions
Overall, our study provides sufficient evidence to suggest that polypharmacy is associated with poorer objective cognitive performance in MS. Furthermore, our results point to the DBI as a useful tool for predicting cognition based on an individual’s medication list. Broadly, clinicians and researchers should account for polypharmacy and anticholinergic effects when evaluating cognition in MS. Tools such as the DBI can allow for quick calculation of anticholinergic burden, which may be clinically addressed by performing a medication review with patients. Although the complex issue of polypharmacy in MS warrants further study, the current findings provide a springboard for future research and clinical considerations.